

Current concepts of metastasis in melanoma
- PMID: 19649148
- PMCID: PMC2601641
- DOI: 10.1586/17469872.3.5.569
Current concepts of metastasis in melanoma
Abstract
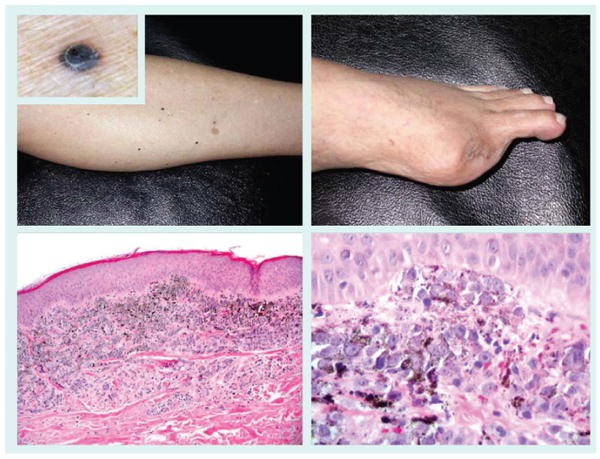
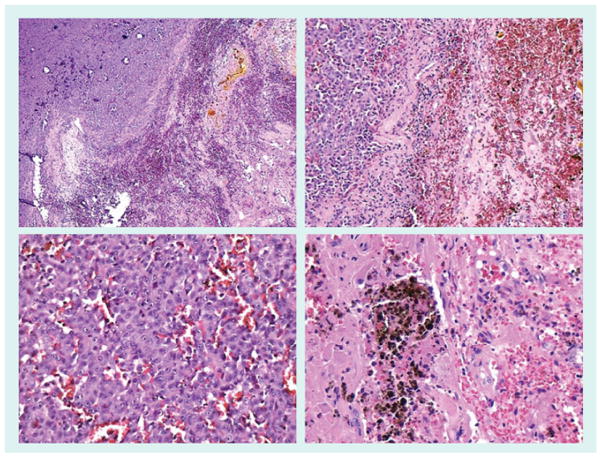
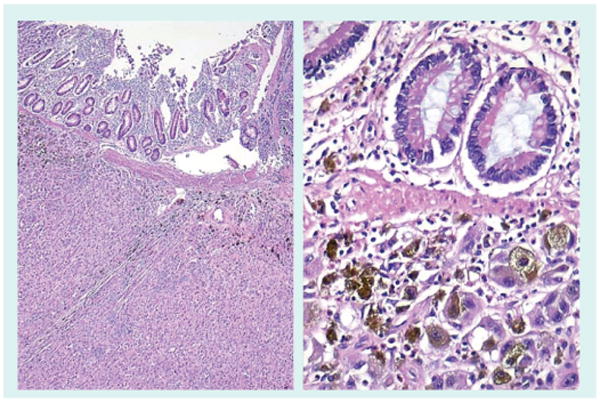
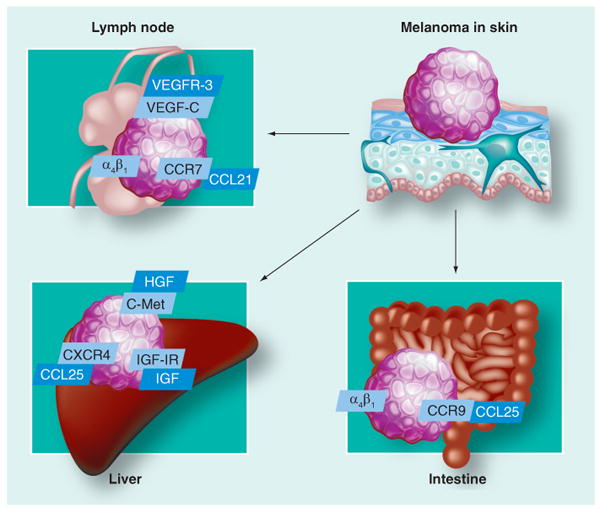
The main cause of death in melanoma patients is widespread metastases. Staging of melanoma is based on the primary tumor thickness, ulceration, lymph node and distant metastases. Metastases develop in regional lymph nodes, as satellite or in-transit lesions, or in distant organs. Lymph flow and chemotaxis is responsible for the homing of melanoma cells to different sites. Standard pathologic evaluation of sentinel lymph nodes fails to find occult melanoma in a significant proportion of cases. Detection of small numbers of malignant melanoma cells in these and other sites, such as adjacent to the primary site, bone marrow or the systemic circulation, may be enhanced by immunohistochemistry, reverse transcription PCR, evaluation of lymphatic vessel invasion and proteomics. In the organs to which melanoma cells metastasize, extravasation of melanoma cells is regulated by adhesion molecules, matrix metalloproteases, chemokines and growth factors. Melanoma cells may travel along external vessel lattices. After settling in the metastatic sites, melanoma cells develop mechanisms that protect them against the attack of the immune system. It is thought that one of the reasons why melanoma cells are especially resistant to killing is the fact that melanocytes (cells from which melanoma cells derive) are resistant to such noxious factors as ultraviolet light and reactive oxygen species. Targeted melanoma therapies are, so far, largely unsuccessful, and new ones, such as adjuvant inhibition of melanogenesis, are under development.
Figures


References
-
- Balch CM, Soong SJ, Atkins MB, et al. An evidence-based staging system for cutaneous melanoma. CA Cancer J Clin. 2004;54(3):131–149. - PubMed
-
- Balch CM, Buzaid AC, Soong SJ et al. Final version of the American Joint Committee on Cancer staging system for cutaneous melanoma. J Clin Oncol. 2001;19(16):3635–3648. - PubMed
-
• Current melanoma staging system.
-
- Bastian BC, Kashani-Sabet M, Hamm H, et al. Gene amplifications characterize acral melanoma and permit the detection of occult tumor cells in the surrounding skin. Cancer Res. 2000;60(7):1968–1973. - PubMed
Website
-
- American Cancer Society; GA, USA: 2008. Cancer facts and figures 2007. www.cancer.org/downloads/STT/CAFF2007PWSecured.pdf.
Grants and funding
LinkOut - more resources
Full Text Sources