

Feasibility of NIRS in the neurointensive care unit: a pilot study in stroke using physiological oscillations
- PMID: 19649749
- PMCID: PMC2782535
- DOI: 10.1007/s12028-009-9254-4
Feasibility of NIRS in the neurointensive care unit: a pilot study in stroke using physiological oscillations
Abstract
Introduction: Near-infrared spectroscopy (NIRS) is a non-invasive, real-time bedside modality sensitive to changes in cerebral perfusion and oxygenation and is highly sensitive to physiological oscillations at different frequencies. However, the clinical feasibility of NIRS remains limited, partly due to concerns regarding NIRS signal quantification, which relies on mostly arbitrary assumptions on hemoglobin concentrations and tissue layers. In this pilot study comparing stroke patients to healthy controls, we explored the utility of the interhemispheric correlation coefficient (IHCC) during physiological oscillations in detecting asymmetry in hemispheric microvascular hemodynamics.
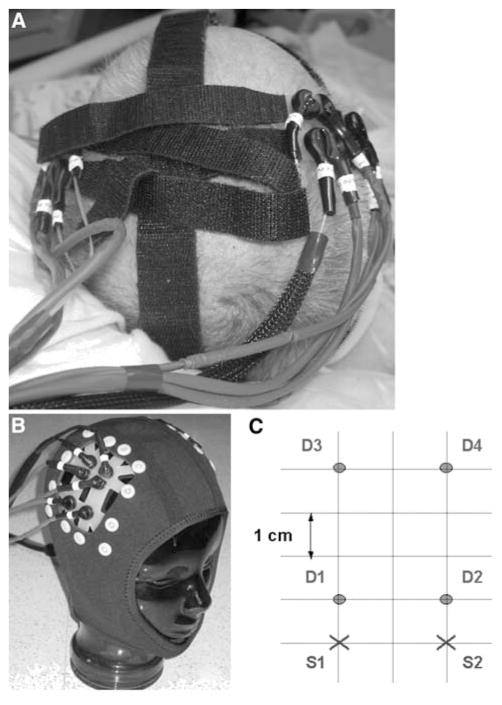
Methods: Using bi-hemispheric continuous-wave NIRS, 12 patients with hemispheric strokes and 9 controls were measured prospectively. NIRS signal was band-pass filtered to isolate cardiac (0.7-3 Hz) and respiratory (0.15-0.7 Hz) oscillations. IHCCs were calculated in both oscillation frequency bands. Using Fisher's Z-transform for non-Gaussian distributions, the IHCC during cardiac and respiratory oscillations were compared between both groups.
Results: Nine patients and nine controls had data of sufficient quality to be included in the analysis. The IHCCs during cardiac and respiratory oscillations were significantly different between patients versus controls (cardiac 0.79 +/- 0.18 vs. 0.94 +/- 0.07, P = 0.025; respiratory 0.24 +/- 0.28 vs. 0.59 +/- 0.3; P = 0.016).
Conclusions: Computing the IHCC during physiological cardiac and respiratory oscillations may be a new NIRS analysis technique to quantify asymmetric microvascular hemodynamics in stroke patients in the neurocritical care unit. It allows each subject to serve as their own control obviating the need for arbitrary assumptions on absolute hemoglobin concentration. Future clinical applications may include rapid identification of patients with ischemic brain injury in the pre-hospital setting. This promising new analysis technique warrants further validation.
Figures


References
-
- Jobsis FF. Noninvasive, infrared monitoring of cerebral and myocardial oxygen sufficiency and circulatory parameters. Science. 1977;198(4323):1264–7. - PubMed
-
- Meek JH, Elwell CE, Khan MJ, et al. Regional changes in cerebral haemodynamics as a result of a visual stimulus measured by near infrared spectroscopy. Proc Biol Sci. 1995;261(1362):351–6. - PubMed
-
- Watanabe E, Maki A, Kawaguchi F, et al. Non-invasive assessment of language dominance with near-infrared spectroscopic mapping. Neurosci Lett. 1998;256(1):49–52. - PubMed
-
- Franceschini MA, Toronov V, Filiaci ME, Gratton E, Fantini S. On-line optical imaging of the human brain with 160-ms temporal resolution. Opt Express. 2000;6:49–57. - PubMed
-
- Kotilahti K, Nissila I, Huotilainen M, et al. Bilateral hemodynamic responses to auditory stimulation in newborn infants. Neuroreport. 2005;16(12):1373–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
