

Direct evidence of mesenchymal stem cell tropism for tumor and wounding microenvironments using in vivo bioluminescent imaging
- PMID: 19650040
- PMCID: PMC4160730
- DOI: 10.1002/stem.187
Direct evidence of mesenchymal stem cell tropism for tumor and wounding microenvironments using in vivo bioluminescent imaging
Abstract
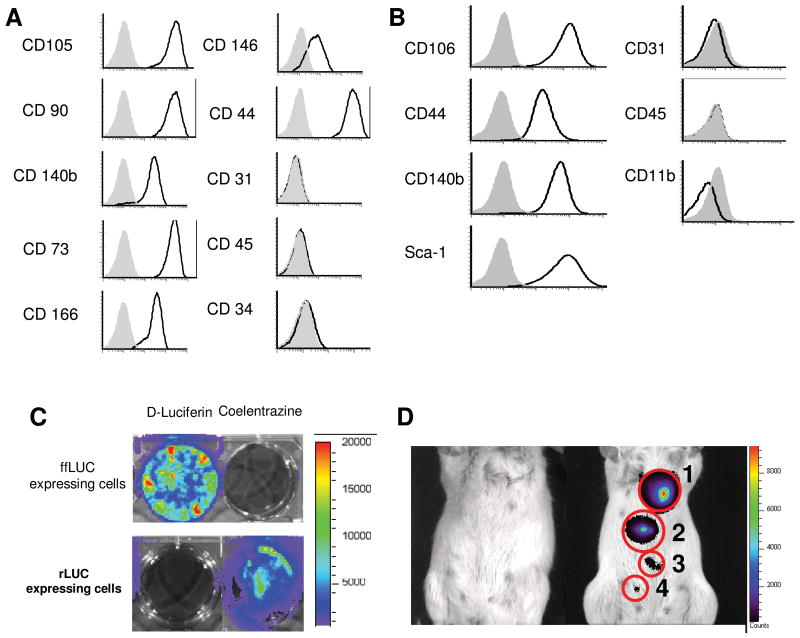
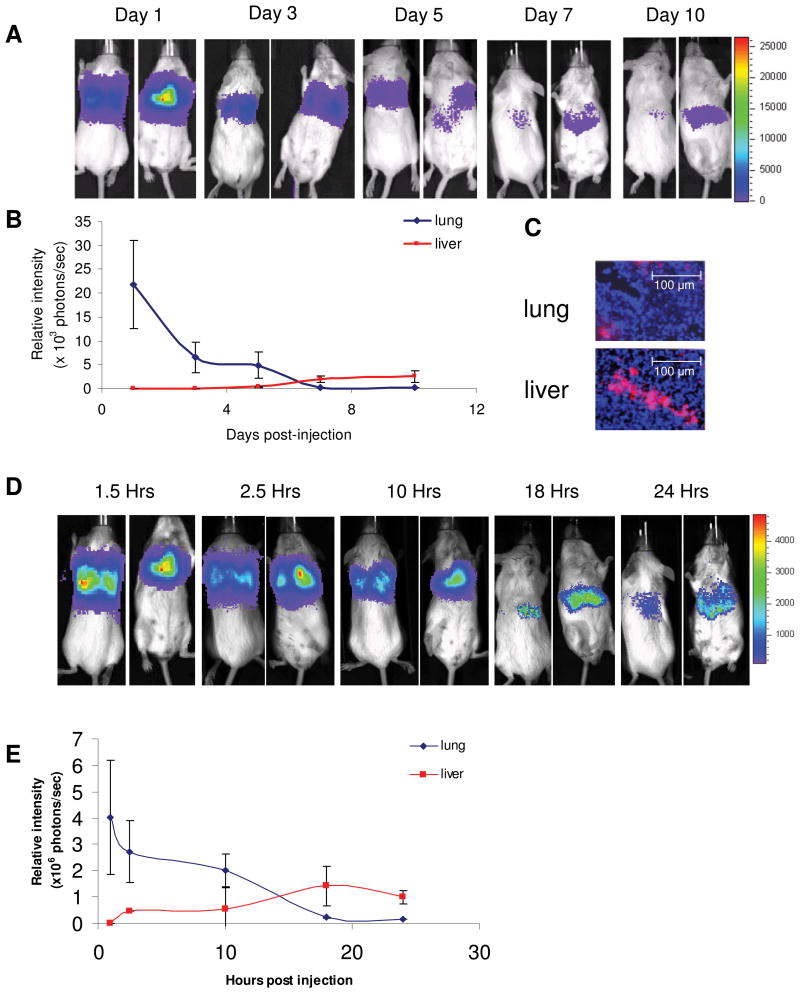
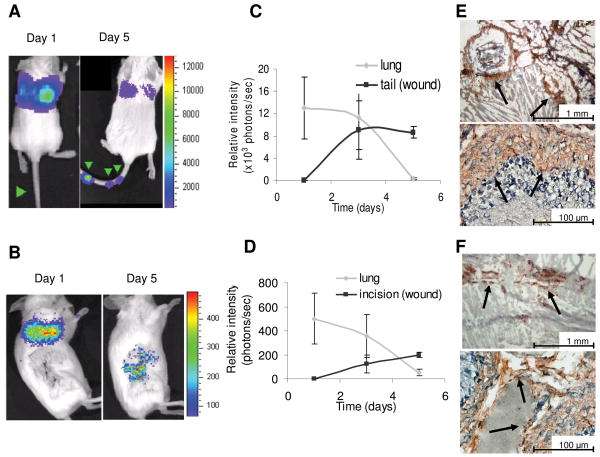
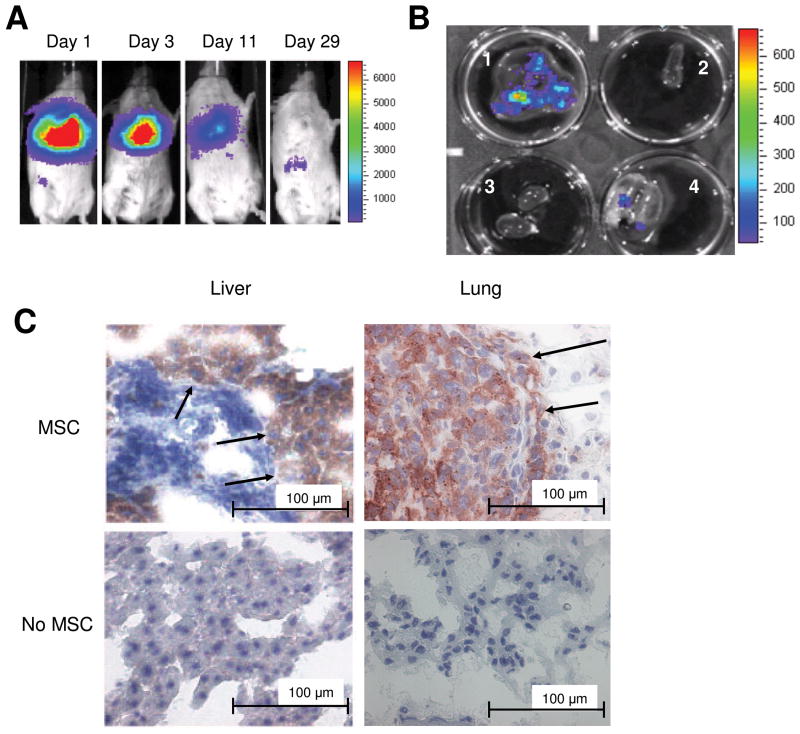
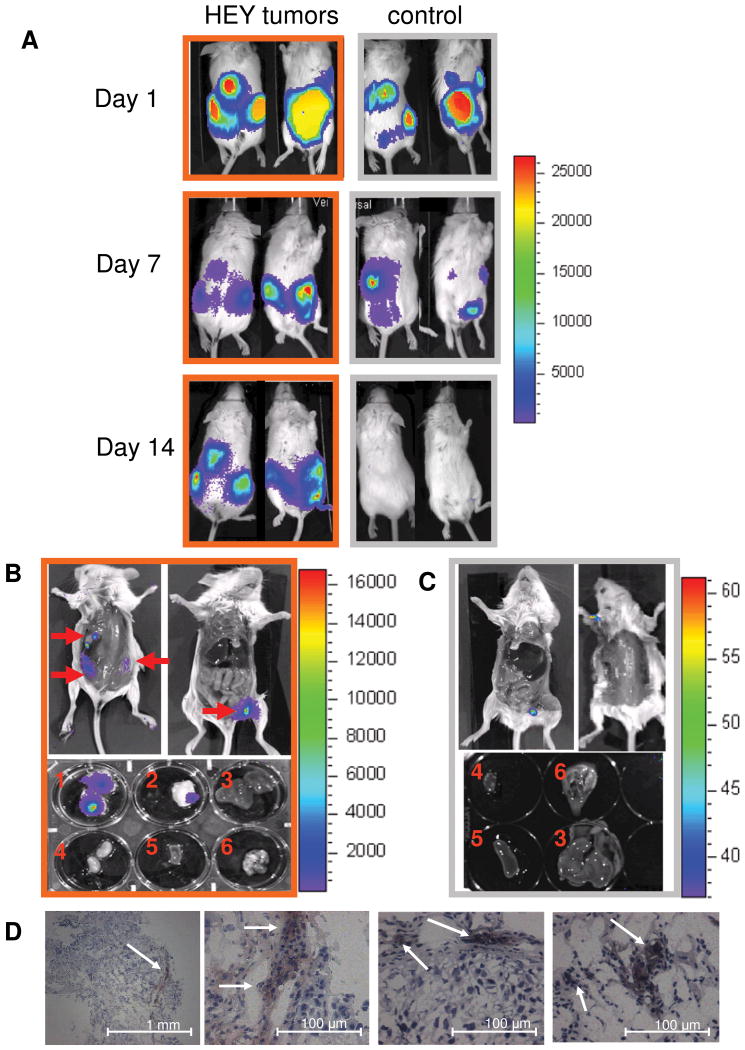
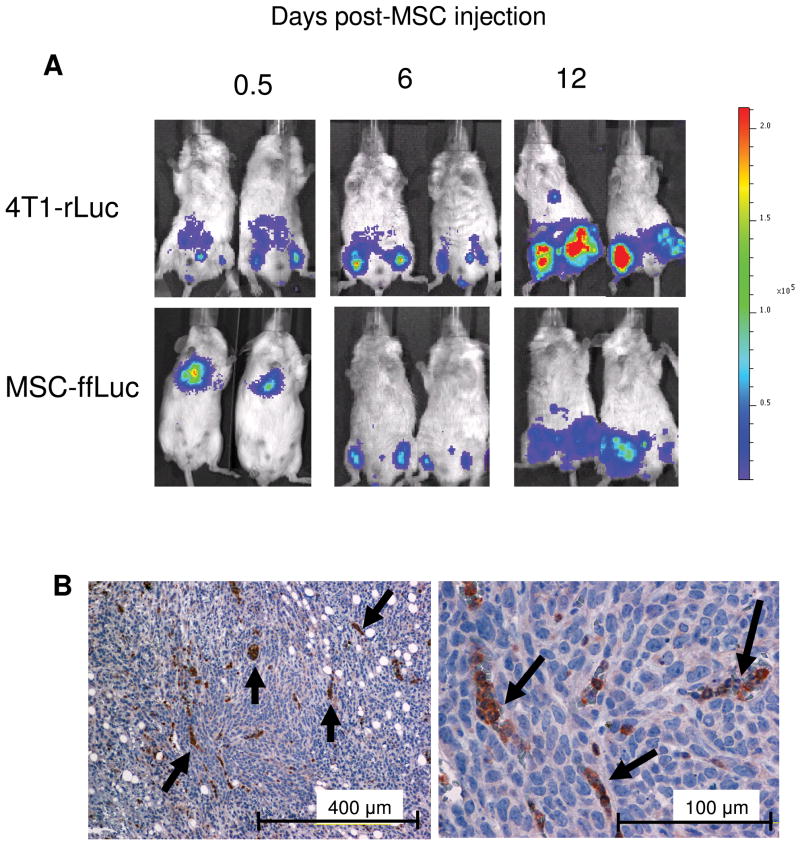
Multipotent mesenchymal stromal/stem cells (MSC) have shown potential clinical utility. However, previous assessments of MSC behavior in recipients have relied on visual detection in host tissue following sacrifice, failing to monitor in vivo MSC dispersion in a single animal and limiting the number of variables that can be observed concurrently. In this study, we used noninvasive, in vivo bioluminescent imaging to determine conditions under which MSC selectively engraft in sites of inflammation. MSC modified to express firefly luciferase (ffLuc-MSC) were injected into healthy mice or mice bearing inflammatory insults, and MSC localization was followed with bioluminescent imaging. The inflammatory insults investigated included cutaneous needle-stick and surgical incision wounds, as well as xenogeneic and syngeneic tumors. We also compared tumor models in which MSC were i.v. or i.p. delivered. Our results demonstrate that ffLuc-expressing human MSC (hMSC) systemically delivered to nontumor-bearing animals initially reside in the lungs, then egress to the liver and spleen, and decrease in signal over time. However, hMSC in wounded mice engraft and remain detectable only at injured sites. Similarly, in syngeneic and xenogeneic breast carcinoma-bearing mice, bioluminescent detection of systemically delivered MSC revealed persistent, specific colocalization with sites of tumor development. This pattern of tropism was also observed in an ovarian tumor model in which MSC were i.p. injected. In this study, we identified conditions under which MSC tropism and selective engraftment in sites of inflammation can be monitored by bioluminescent imaging over time. Importantly, these consistent findings were independent of tumor type, immunocompetence, and route of MSC delivery.
Figures
References
-
- Nakamizo A, Marini F, Amano T, et al. Human bone marrow-derived mesenchymal stem cells in the treatment of gliomas. Cancer Res. 2005;65:3307–3318. - PubMed
-
- Studeny M, Marini FC, Dembinski JL, et al. Mesenchymal stem cells: potential precursors for tumor stroma and targeted-delivery vehicles for anticancer agents. J Natl Cancer Inst. 2004;96:1593–1603. - PubMed
-
- Sasaki M, Abe R, Fujita Y, et al. Mesenchymal stem cells are recruited into wounded skin and contribute to wound repair by transdifferentiation into multiple skin cell type. J Immunol. 2008;180:2581–2587. - PubMed
-
- Satake K, Lou J, Lenke LG. Migration of mesenchymal stem cells through cerebrospinal fluid into injured spinal cord tissue. Spine. 2004;29:1971–1979. - PubMed
-
- Neuhuber B, Timothy Himes B, Shumsky JS, et al. Axon growth and recovery of function supported by human bone marrow stromal cells in the injured spinal cord exhibit donor variations. Brain Res. 2005;1035:73–85. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
