

Prospective study of [18F]fluorodeoxyglucose positron emission tomography/computed tomography for staging of muscle-invasive bladder carcinoma
- PMID: 19652070
- PMCID: PMC4035361
- DOI: 10.1200/JCO.2008.20.6722
Prospective study of [18F]fluorodeoxyglucose positron emission tomography/computed tomography for staging of muscle-invasive bladder carcinoma
Abstract
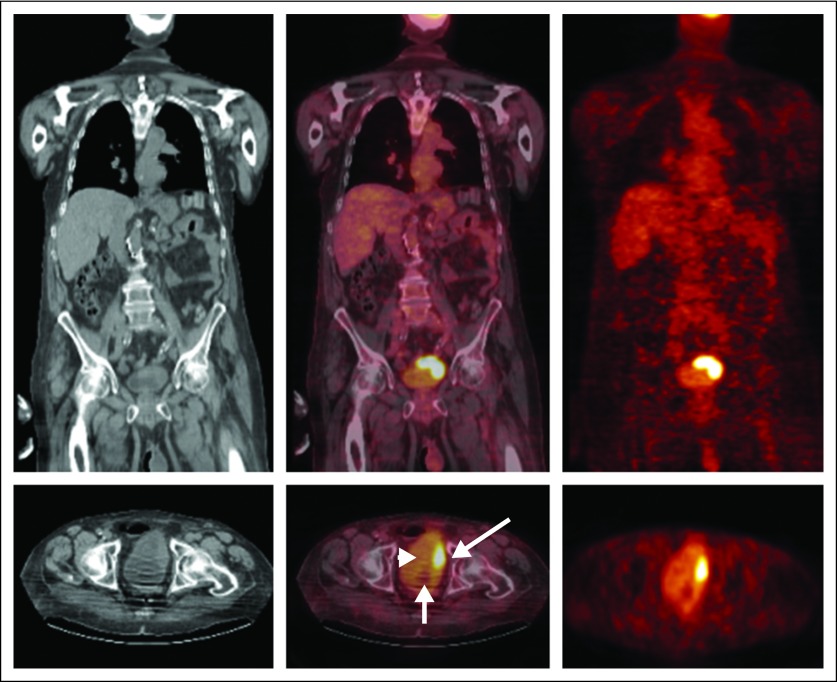
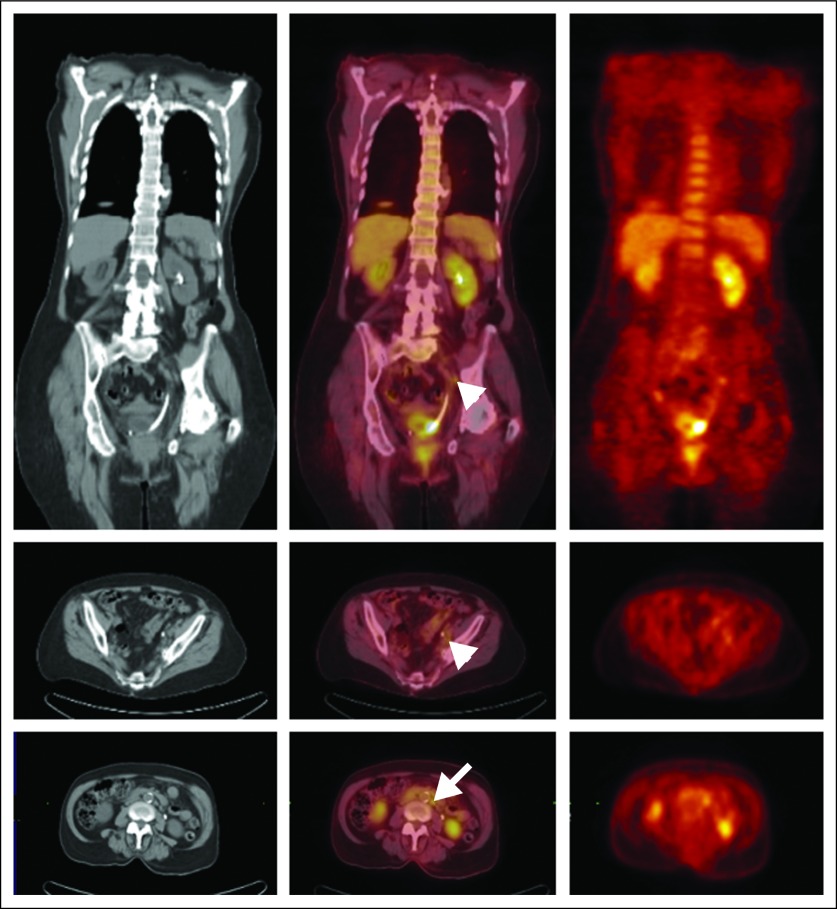
Purpose: Novel imaging modalities are needed to detect occult metastatic disease in bladder carcinoma. Patients with regional lymphatic spread could be targeted for neoadjuvant chemotherapy, and patients with distant metastatic disease could be spared the unnecessary morbidity of radical cystectomy. Herein, we report a prospective study of positron emission tomography/computed tomography (PET/CT) with [(18)F]fluorodeoxyglucose (FDG) in patients undergoing radical cystectomy for cT2-3N0M0 urothelial carcinoma of the bladder.
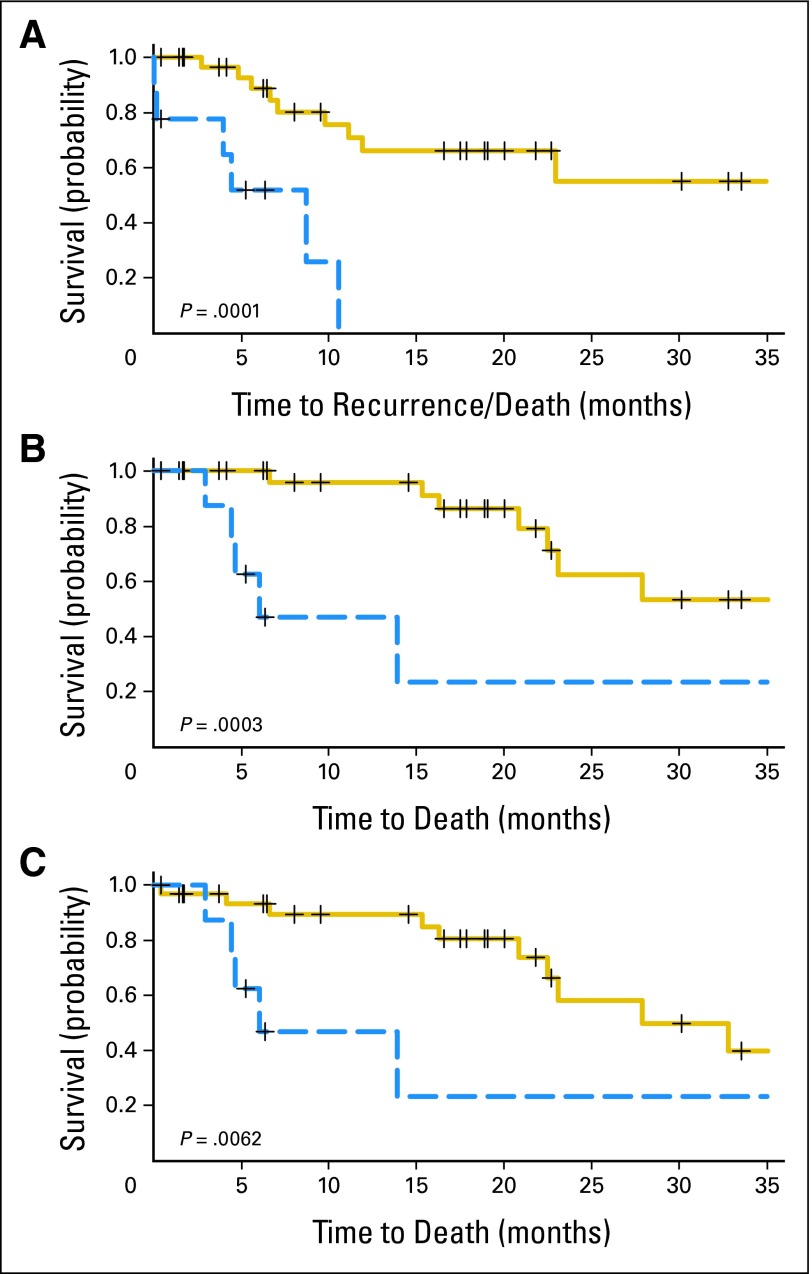
Methods: Forty-three chemotherapy-naïve patients underwent FDG-PET/CT before planned cystectomy. All had negative conventional CT and bone scintigraphy before enrollment. Positive FDG-PET/CT was confirmed by percutaneous biopsy or open surgical exploration, whereas negative FDG-PET/CT was confirmed by complete lymphadenectomy. Recurrence-free survival (RFS), disease-specific survival (DSS), and overall survival (OS) were described using the Kaplan-Meier method and compared using log-rank test.
Results: Median follow-up was 14.9 months (range, 0.4 to 46.1 months). One patient who did not undergo lymphadenectomy was excluded from the pathology data analysis (n = 42), whereas another patient who failed to return for follow-up was excluded from survival analysis (n = 42). FDG-PET/CT demonstrated a positive predictive value of 78% (seven of nine), a negative predictive value of 91% (30 of 33), sensitivity of 70% (seven of 10), and specificity of 94% (30 of 32). RFS, DSS, and OS were all significantly poorer in the patients with positive FDG-PET/CT than in those with negative FDG-PET/CT.
Conclusion: FDG-PET/CT detected occult metastatic disease in seven of 42 patients with negative conventional preoperative evaluations. PET findings were strongly correlated with survival. As such, FDG-PET/CT may help in making treatment decisions before radical cystectomy.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Bellmunt J, Albiol S, Suarez C, et al. Optimizing therapeutic strategies in advanced bladder cancer: Update on chemotherapy and the role of targeted agents. Crit Rev Oncol Hematol. 2009;69:211–222. - PubMed
-
- Stein JP, Lieskovsky G, Cote R, et al. Radical cystectomy in the treatment of invasive bladder cancer: Long-term results in 1,054 patients. J Clin Oncol. 2001;19:666–675. - PubMed
-
- Neoadjuvant cisplatin, methotrexate, and vinblastine chemotherapy for muscle-invasive bladder cancer: A randomised controlled trial—International collaboration of trialists. Lancet. 1999;354:533–540. - PubMed
-
- Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. 2003;349:859–866. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
