Buprenorphine medication versus voucher contingencies in promoting abstinence from opioids and cocaine
- PMID: 19653788
- PMCID: PMC2852314
- DOI: 10.1037/a0016597
Buprenorphine medication versus voucher contingencies in promoting abstinence from opioids and cocaine
Abstract
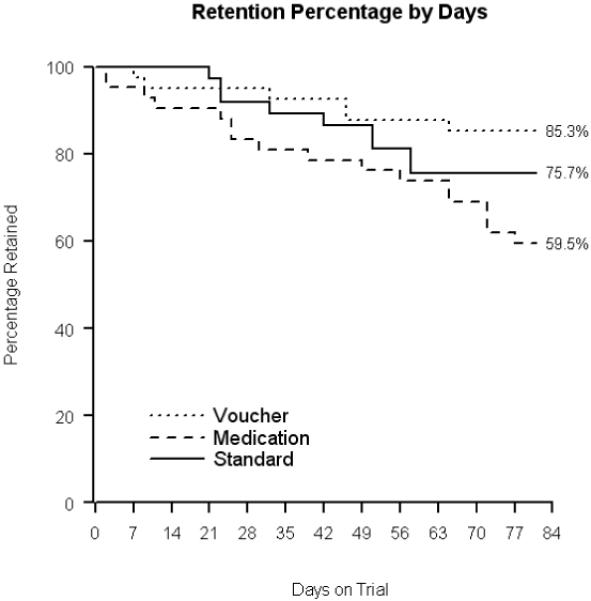
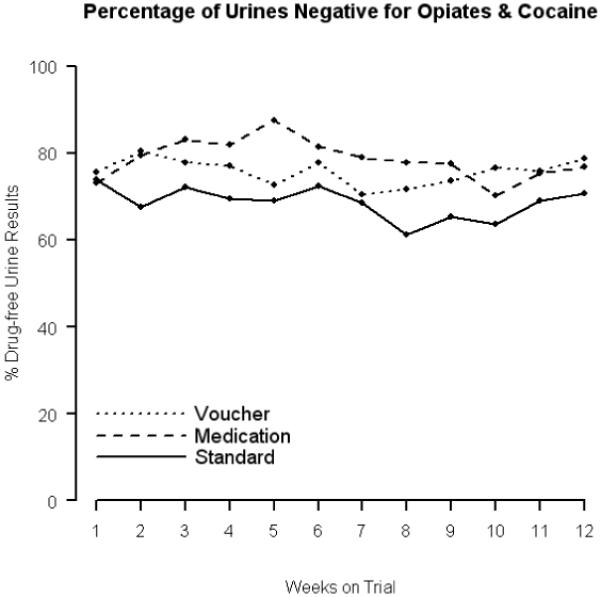
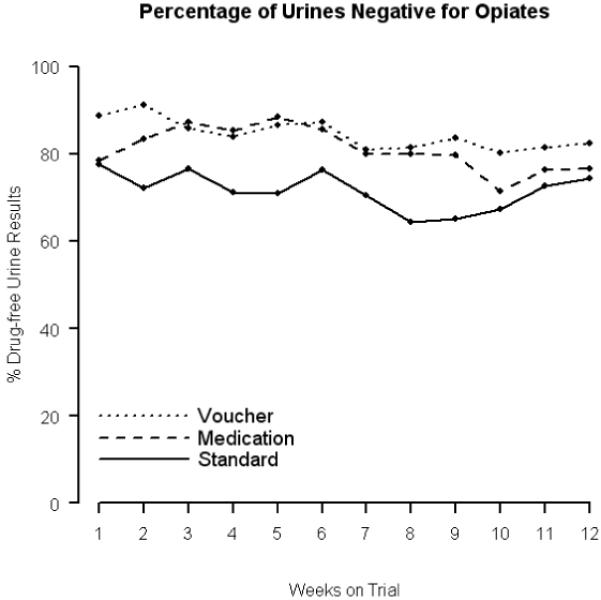
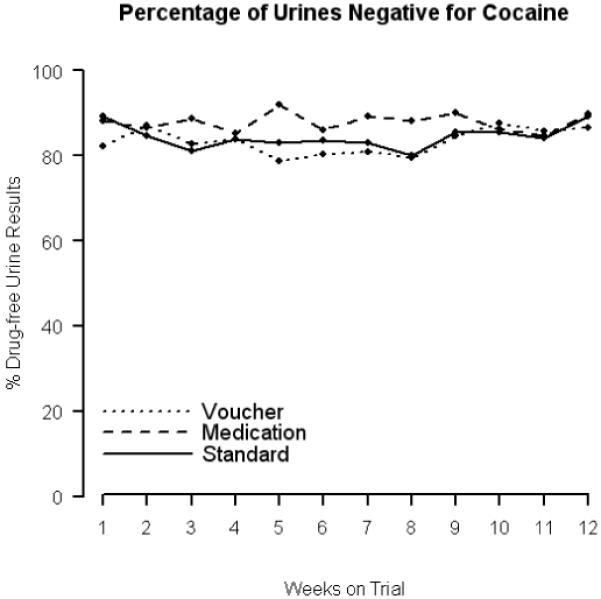
During a 12-week intervention, opioid dependent participants (N = 120) maintained on thrice-a-week (M, W, F) buprenorphine plus therapist and computer-based counseling were randomized to receive: (a) medication contingencies (MC = thrice weekly dosing schedule vs. daily attendance and single-day 50% dose reduction imposed upon submission of an opioid and/or cocaine positive urine sample); (b) voucher contingency (VC = escalating schedule for opioid and/or cocaine negative samples with reset for drug-positive samples); or (c) standard care (SC), with no programmed consequences for urinalysis results. VC resulted in better 12-week retention (85%) compared to MC (58%; p = 0.009), but neither differed from SC (76% retained). After adjusting for baseline differences in employment, and compared to SC, the MC group achieved 1.5 more continuous weeks of combined opioid/cocaine abstinence (p = 0.030), while the VC group had 2 more total weeks of abstinence (p = 0.048). Drug use results suggest that both the interventions were efficacious, with effects primarily in opioid rather than cocaine test results. Findings should be interpreted in light of the greater attrition associated with medication-based contingencies versus the greater monetary costs of voucher-based contingencies.
2009 APA, all rights reserved.
Figures
References
-
- Aickin M. A program for balancing the allocation of subjects to treatment in a clinical trial. Computers and Biomedical Research. 1982;15:519–524. - PubMed
-
- Amass L, Bickel WK, Crean JP, Blake J, Higgins ST. Alternate-day buprenorphine dosing is preferred to daily dosing by opioid-dependent humans. Psychopharmacology. 1998;136:217–225. - PubMed
-
- Amass L, Bickel WK, Higgins ST, Badger GJ. Alternate-day dosing during buprenorphine treatment of opioid dependence. Life Sciences. 1994;54:1215–1228. - PubMed
-
- American Psychiatric Association . Diagnostic and Statistical manual of Mental Disorders. 4th ed. Author; Washington, DC: 1994.
-
- Bickel WK, Amass L, Higgins ST, Badger GJ, Esch R. Effects of adding behavioral treatment to opioid detoxification with buprenorphine. Journal of Consulting and Clinical Psychology. 1997;65:803–810. - PubMed