

Single ray amputation for tumors of the hand
- PMID: 19655212
- PMCID: PMC2853661
- DOI: 10.1007/s11999-009-1019-z
Single ray amputation for tumors of the hand
Abstract
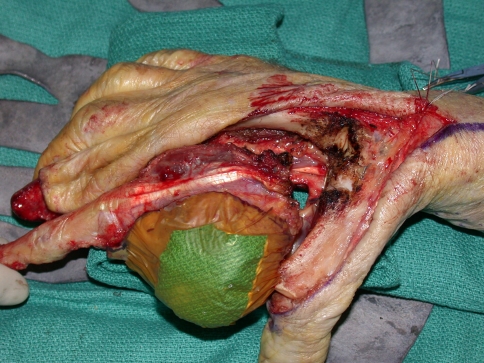
Single ray amputation after hand trauma or infection can result in good aesthetic and functional outcomes. The role of this procedure in the management of aggressive benign or malignant hand tumors has been described only in case reports and small case series. We retrospectively reviewed the records of all 25 patients who underwent single ray amputations at our center during a 10-year period; there were seven index, five middle, six ring, and seven small ray amputations performed. The minimum followup was 2 months (mean, 36 months; range, 2-120 months), with four patients having a followup of 1 year or less. No patients had local recurrences, although two patients had positive resection margins. One underwent repeat resection followed by radiotherapy. The other was treated with radiotherapy alone, as local tumor control would have required a hand amputation. Functional assessment based on the Musculoskeletal Tumor Society staging system showed an average of 27.5 (range, 21-30). Patients who underwent perioperative radiotherapy experienced a decrease in functional ability. Grip strength was an average of 66% (range, 38%-100%) of the contralateral side. Our study suggests single ray amputation for hand tumors has a low local recurrence rate and high functional scores. However, function can be compromised by radiotherapy and a decrease in grip strength by a mean of 34% is to be expected.
Level of evidence: Level IV, case series. See Guidelines for Authors for a complete description of levels of evidence.
Figures



References
-
- Enneking WF, Dunham W, Gebhardt MC, Malawar M, Pritchard DJ. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin Orthop Relat Res. 1993;286:241–246. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
