

Defining the relationship between Plasmodium falciparum parasite rate and clinical disease: statistical models for disease burden estimation
- PMID: 19656373
- PMCID: PMC2746234
- DOI: 10.1186/1475-2875-8-186
Defining the relationship between Plasmodium falciparum parasite rate and clinical disease: statistical models for disease burden estimation
Abstract
Background: Clinical malaria has proven an elusive burden to enumerate. Many cases go undetected by routine disease recording systems. Epidemiologists have, therefore, frequently defaulted to actively measuring malaria in population cohorts through time. Measuring the clinical incidence of malaria longitudinally is labour-intensive and impossible to undertake universally. There is a need, therefore, to define a relationship between clinical incidence and the easier and more commonly measured index of infection prevalence: the "parasite rate". This relationship can help provide an informed basis to define malaria burdens in areas where health statistics are inadequate.
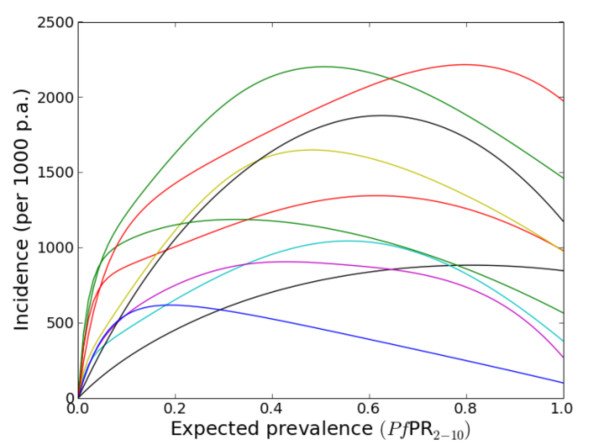
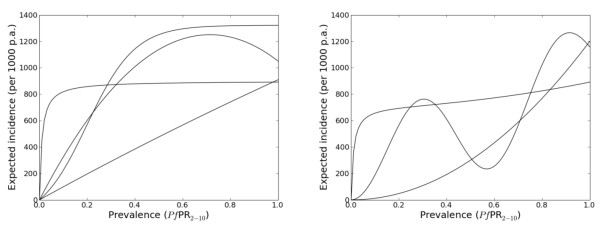
Methods: Formal literature searches were conducted for Plasmodium falciparum malaria incidence surveys undertaken prospectively through active case detection at least every 14 days. The data were abstracted, standardized and geo-referenced. Incidence surveys were time-space matched with modelled estimates of infection prevalence derived from a larger database of parasite prevalence surveys and modelling procedures developed for a global malaria endemicity map. Several potential relationships between clinical incidence and infection prevalence were then specified in a non-parametric Gaussian process model with minimal, biologically informed, prior constraints. Bayesian inference was then used to choose between the candidate models.
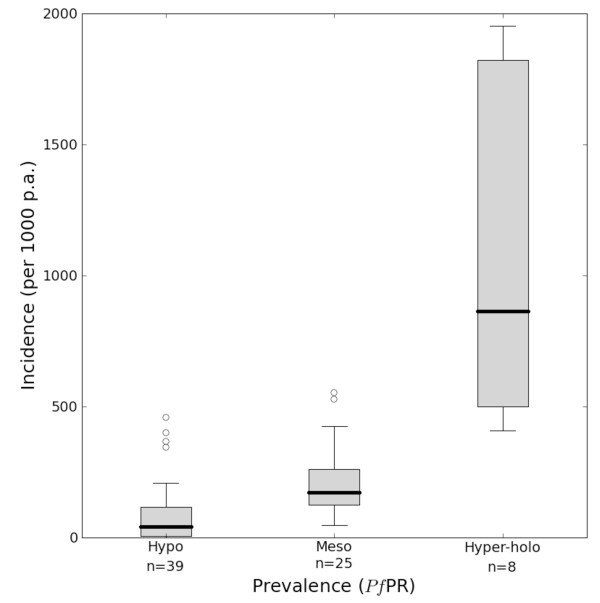
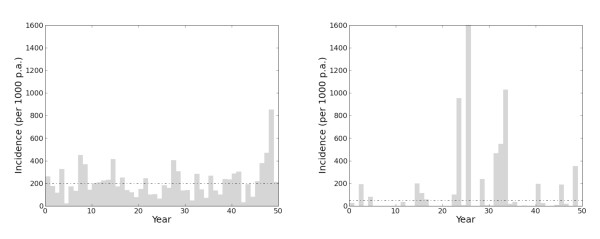
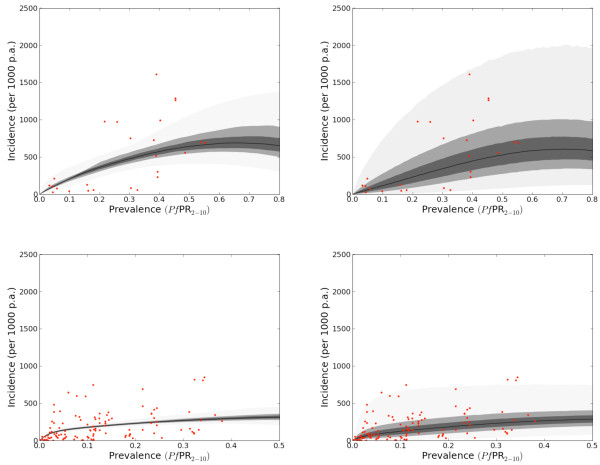
Results: The suggested relationships with credible intervals are shown for the Africa and a combined America and Central and South East Asia regions. In both regions clinical incidence increased slowly and smoothly as a function of infection prevalence. In Africa, when infection prevalence exceeded 40%, clinical incidence reached a plateau of 500 cases per thousand of the population per annum. In the combined America and Central and South East Asia regions, this plateau was reached at 250 cases per thousand of the population per annum. A temporal volatility model was also incorporated to facilitate a closer description of the variance in the observed data.
Conclusion: It was possible to model a relationship between clinical incidence and P. falciparum infection prevalence but the best-fit models were very noisy reflecting the large variance within the observed opportunistic data sample. This continuous quantification allows for estimates of the clinical burden of P. falciparum of known confidence from wherever an estimate of P. falciparum prevalence is available.
Figures
References
-
- Bruce-Chwatt LJ. Malaria in African infants and children in Southern Nigeria. Ann Trop Med Parasitol. 1952;46:173–200. - PubMed
-
- Roca-Feltrer A, Carneiro I, Armstrong Schellenberg JR. Estimates of the burden of malaria morbidity in Africa in children under the age of 5 years. Trop Med Int Health. 2008;13:771–783. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
