

The metabolic syndrome in children and adolescents
- PMID: 19657446
- PMCID: PMC2720902
- DOI: 10.1093/pch/10.1.41
The metabolic syndrome in children and adolescents
Abstract
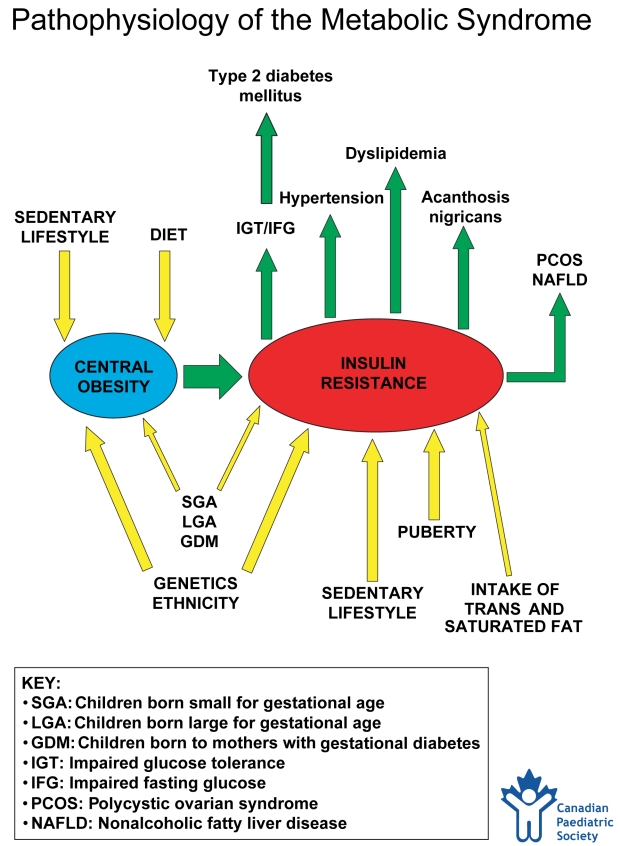
The metabolic syndrome is a constellation of metabolic abnormalities that result in an increased risk for type 2 diabetes mellitus and cardiovascular disease in adults. It emerges when a person's predisposition for insulin resistance is worsened by increasing central obesity and is largely confined to the overweight population. The United States National Cholesterol Education Program's Adult Treatment Panel III report proposed a set of criteria for the clinical diagnosis of metabolic syndrome in the adult population. A uniform definition for the paediatric population is lacking. Despite this, several studies have demonstrated that features of the syndrome develop in childhood and that the syndrome is present in up to 30% of obese children (body mass index at or above the 95th percentile). Ninety per cent of obese children meet at least one of the five criteria. The degree of abnormality is related to the body mass index, waist circumference and fasting insulin levels. There appears to be a genetic predisposition to the development of the syndrome and certain ethnic groups are at increased risk. The intrauterine environment also appears to play a role. Insulin resistance should be targeted for treatment through exercise and dietary intervention. The role of pharmacotherapeutic agents remains unclear. A uniform definition of the metabolic syndrome for paediatric patients needs to be created. Early intervention should be instituted because many of the features of the syndrome track from childhood into adulthood.
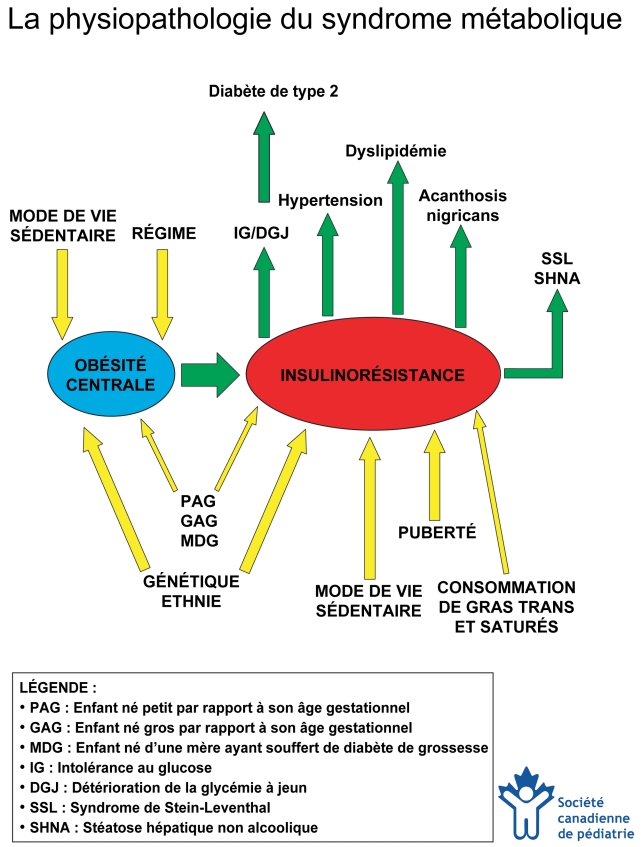
Le syndrome métabolique est une constellation d’anomalies métaboliques qui entraînent une augmentation du risque de diabète non insulinodépendant et de maladies cardiovasculaires chez les adultes. Il émerge lorsque la prédisposition d’un individu à l’insulinorésistance est aggravée par une obésité centrale croissante, et il est largement confiné à la population qui fait de l’embonpoint. Le rapport du groupe III de traitement aux adultes du National Cholesterol Education Program des États-Unis a proposé une série de critères pour parvenir au diagnostic clinique du syndrome métabolique dans la population adulte. Il n’existe pas de définition uniforme pour la population pédiatrique. Malgré tout, plusieurs études ont démontré que des caractéristiques du syndrome se déclarent pendant l’enfance et que jusqu’à 30 % des enfants obèses (dont l’indice de masse corporelle est égal ou supérieur au 95e percentile) souffrent du syndrome. Quatre-vingt-dix pour cent des enfants obèses respectent au moins l’un des cinq critères. Le degré d’anomalie est relié à l’indice de masse corporelle, à la circonférence de la taille et aux taux d’insuline à jeun. Il semble exister une prédisposition génétique à l’apparition du syndrome, et certains groupes ethniques y sont plus vulnérables. L’environnement intra-utérin semble également avoir un rôle à jouer. L’insulinorésistance devrait être ciblée pour un traitement par l’exercice et une intervention diététique. Le rôle de la pharmacothérapie demeure incertain. Une définition uniforme du syndrome métabolique s’impose pour la population pédiatrique. Une intervention précoce devrait être appliquée, car bon nombre des caractéristiques du syndrome sont maintenues de l’enfance à l’âge adulte.
Keywords: Cardiovascular disease; Insulin resistance; Metabolic syndrome; Obesity; Type 2 diabetes.
Figures
References
-
- Alexander CM, Landsman PB, Teutsch SM, Haffner SM. NCEP-defined metabolic syndrome, diabetes, and prevalence of coronary heart disease among NHANES III participants age 50 years and older. Diabetes. 2003;52:1210–4. - PubMed
-
- Isoma B, Almgren P, Tuomi T, et al. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care. 2001;24:683–9. - PubMed
-
- Malik S, Wong ND, Franklin SS, et al. Impact of the metabolic syndrome on mortality from coronary artery disease, cardiovascular disease and all causes in United States adults. Circulation. 2004;110:1245–50. - PubMed
-
- Laaksonen DE, Lakka HM, Niskanen LK, Kaplan GA, Salonen JT, Lakka TA. Metabolic syndrome and development of diabetes mellitus: Application and validation of recently suggested definitions of the metabolic syndrome in a prospective cohort study. Am J Epidemiol. 2002;156:1070–7. - PubMed
-
- Hanson RL, Imperatore G, Vennett PH, Knowler WC. Components of the “metabolic syndrome” and incidence of type 2 diabetes. Diabetes. 2002;51:3120–7. - PubMed
LinkOut - more resources
Full Text Sources