

Comparison of nonsteroidal anti-inflammatory drugs and cyclooxygenase-2 (COX-2) inhibitors use in Australia and Nova Scotia (Canada)
- PMID: 19660008
- PMCID: PMC2732945
- DOI: 10.1111/j.1365-2125.2009.03410.x
Comparison of nonsteroidal anti-inflammatory drugs and cyclooxygenase-2 (COX-2) inhibitors use in Australia and Nova Scotia (Canada)
Abstract
Aims: Cyclooxygenase-2 (COX-2) inhibitors were marketed aggressively and their rapid uptake caused safety concerns and budgetary challenges in Canada and Australia. The objectives of this study were to compare and contrast COX-2 inhibitors and nonselective nonsteroidal anti-inflammatory drug (ns-NSAID) use in Nova Scotia (Canada) and Australia and to identify lessons learned from the two jurisdictions.
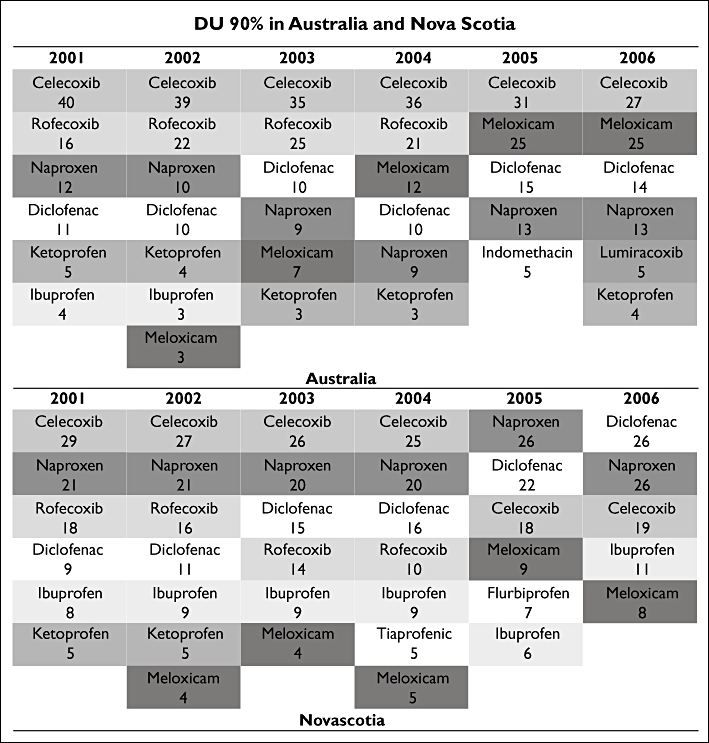
Methods: Ns-NSAID and COX-2 inhibitor Australian prescription data (concession beneficiaries) were downloaded from the Medicare Australia website (2001-2006). Similar Pharmacare data were obtained for Nova Scotia (seniors and those receiving Community services). Defined daily doses per 1000 beneficiaries day(-1) were calculated. COX-2 inhibitors/all NSAIDs ratios were calculated for Australia and Nova Scotia. Ns-NSAIDs were divided into low, moderate and high risk for gastrointestinal side-effects and the proportions of use in each group were determined. Which drugs accounted for 90% of use was also calculated.
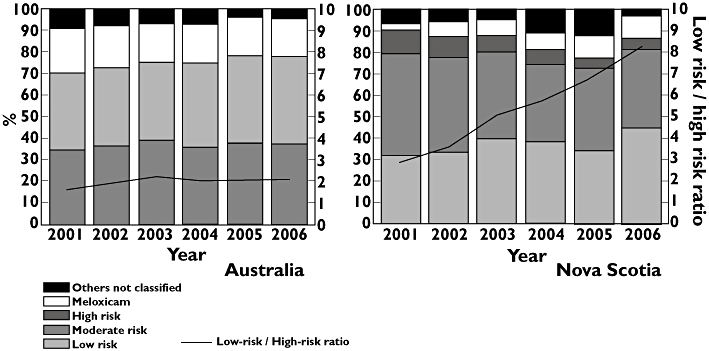
Results: Overall NSAID use was different in Australia and Nova Scotia. However, ns-NSAID use was similar. COX-2 inhibitor dispensing was higher in Australia. The percentage of COX-2 inhibitor prescriptions over the total NSAID use was different in the two countries. High-risk NSAID use was much higher in Australia. Low-risk NSAID prescribing increased in Nova Scotia over time. The low-risk/high-risk ratio was constant throughout over the period in Australia and increased in Nova Scotia.
Conclusions: There are significant differences in Australia and Nova Scotia in use of NSAIDs, mainly due to COX-2 prescribing. Nova Scotia has a higher proportion of low-risk NSAID use. Interventions to provide physicians with information on relative benefits and risks of prescribing specific NSAIDs are needed, including determining their impact.
Figures
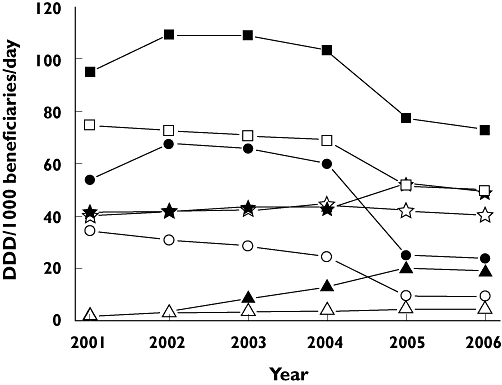
 ); ns-NSAIDs NS (—⋆—); ns-NSAIDs AUS (—⋆—); meloxicam NS (—▵—); meloxicam AUS (—▴—); All NSAIDs NS (—□—); All NSAIDs AUS (
); ns-NSAIDs NS (—⋆—); ns-NSAIDs AUS (—⋆—); meloxicam NS (—▵—); meloxicam AUS (—▴—); All NSAIDs NS (—□—); All NSAIDs AUS ( )
)
 ); meloxicam (
); meloxicam ( ); high risk (
); high risk ( ); moderate risk (
); moderate risk ( ); low risk (
); low risk ( ); Low-risk / High-risk ratio (
); Low-risk / High-risk ratio ( )
)References
-
- Hawkins C, Hanks G. The gastoduodenal toxicity of nonsteroidal anti-inflammatory drugs. A review of the literature. J Pain Symptom Manage. 2000;20:140–51. - PubMed
-
- Jones R. Nonsteroidal anti-inflammatory drug prescribing: past, present, and future. Am J Med. 2001;110:4S–7S. - PubMed
-
- Hermann M, Ruschitzka F. Coxibs, non-steroidal anti-inflammatory drugs and cardiovascular risk. Intern Med J. 2006;36:308–19. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
