

BK virus infection is associated with hematuria and renal impairment in recipients of allogeneic hematopoetic stem cell transplants
- PMID: 19660716
- PMCID: PMC2723723
- DOI: 10.1016/j.bbmt.2009.04.016
BK virus infection is associated with hematuria and renal impairment in recipients of allogeneic hematopoetic stem cell transplants
Abstract
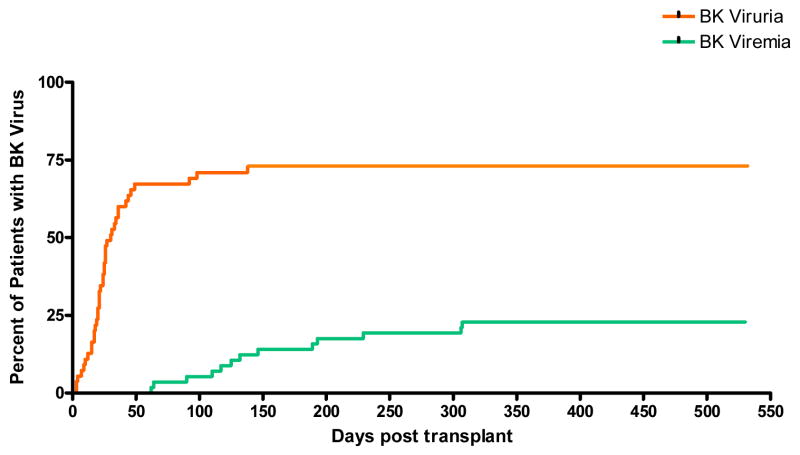
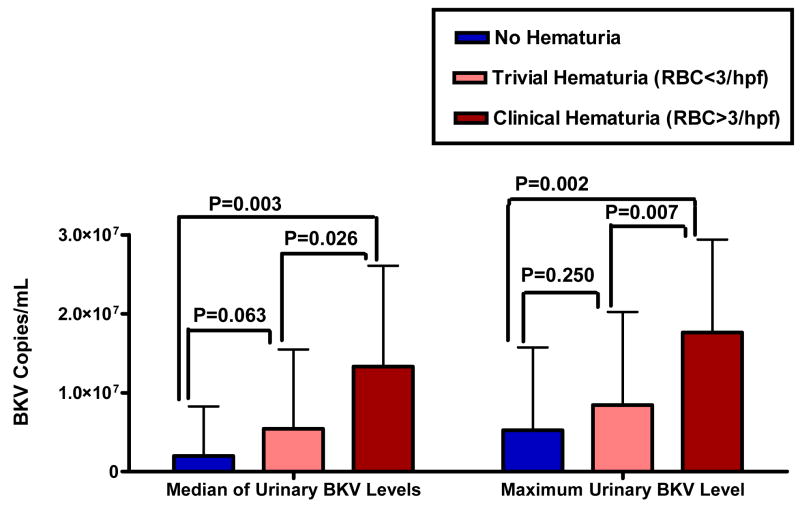
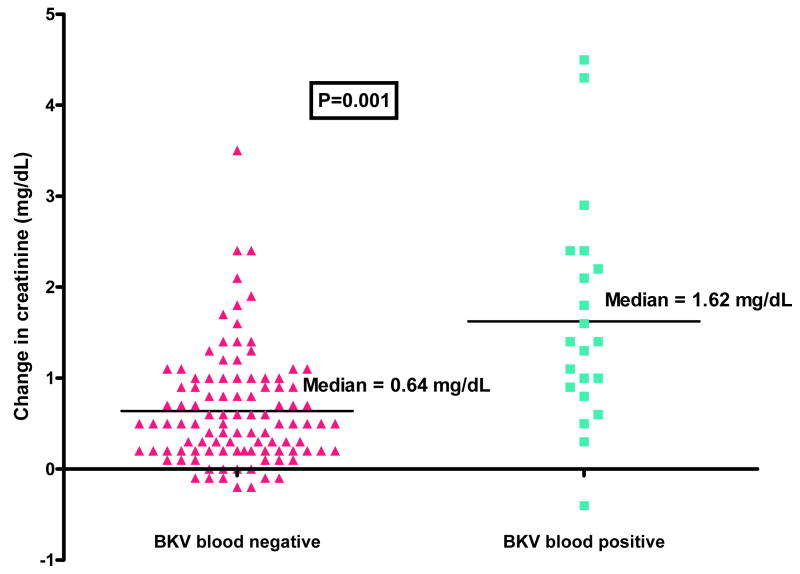
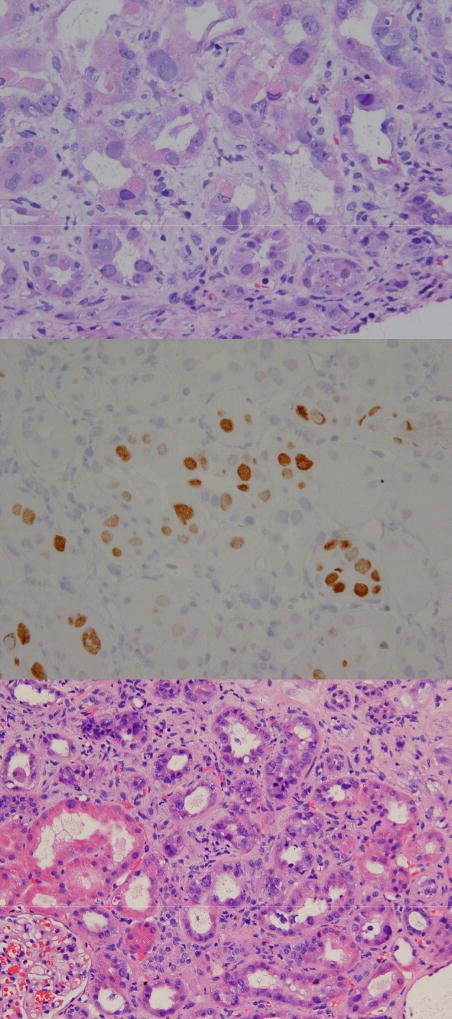
BK virus (BKV) is an important pathogen and cause of nephropathy in renal transplant recipients, but its significance following hematopoetic stem cell transplantation (HSCT) is less well described. We measured blood and urine BKV in 124 allogeneic HSCT patients (67 had undergone prior HSCT [surveillance cohort]; 57 were monitored from transplant day 0 [prospective cohort]). BK viruria was manifest in 64.8% of the patients; 16.9% developed viremia. In the prospective cohort, the median time from transplantation to BK viremia development (128 days) was longer than for viruria (24 days; P < .0001). Among clinical factors (sex, disease, transplant type, alemtuzumab use, cytomegalovirus [CMV] viremia, graft-versus-host disease [GVHD], donor HLA C7 allele), only CMV viremia was more common in patients with BKV infection (P < or = .04). There was a direct relationship between blood and urine BKV levels and the occurrence, and degree, of hematuria (P < or = .03). Finally, BKV infection was analyzed along with other clinical factors in relation to the development of post-HSCT renal impairment. On multivariate analysis, only BK viremia (P=.000002) and alternative-donor transplantation (P=.002) were independent predictors of development of post-HSCT renal impairment, with BK viremia associated with a median 1.62mg/dL rise in creatinine from the pretransplant baseline. Among 8 patients in the surveillance cohort with BK viremia, 2 developed biopsy-proven BKV nephropathy requiring hemodialysis. Investigation of whether prophylaxis against, or treatment of, BKV in the post-HSCT setting mitigates the associated morbidities, especially kidney injury, warrants prospective evaluation.
Figures
References
-
- Hirsch HH, Steiger J. Polyomavirus BK. The Lancet Infectious Diseases. 2003;3:611–623. - PubMed
-
- Fishman JA. BK virus nephropathy--polyomavirus adding insult to injury. [comment] New England Journal of Medicine. 2002;347:527–530. - PubMed
-
- Reploeg MD, Storch GA, Clifford DB. Bk virus: a clinical review. Clinical Infectious Diseases. 2001;33:191–202. - PubMed
-
- Nickeleit V, Mihatsch MJ. Polyomavirus nephropathy in native kidneys and renal allografts: an update on an escalating threat. Transplant International. 2006;19:960–973. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
