

Five year prognosis in patients with angina identified in primary care: incident cohort study
- PMID: 19661139
- PMCID: PMC2722695
- DOI: 10.1136/bmj.b3058
Five year prognosis in patients with angina identified in primary care: incident cohort study
Abstract
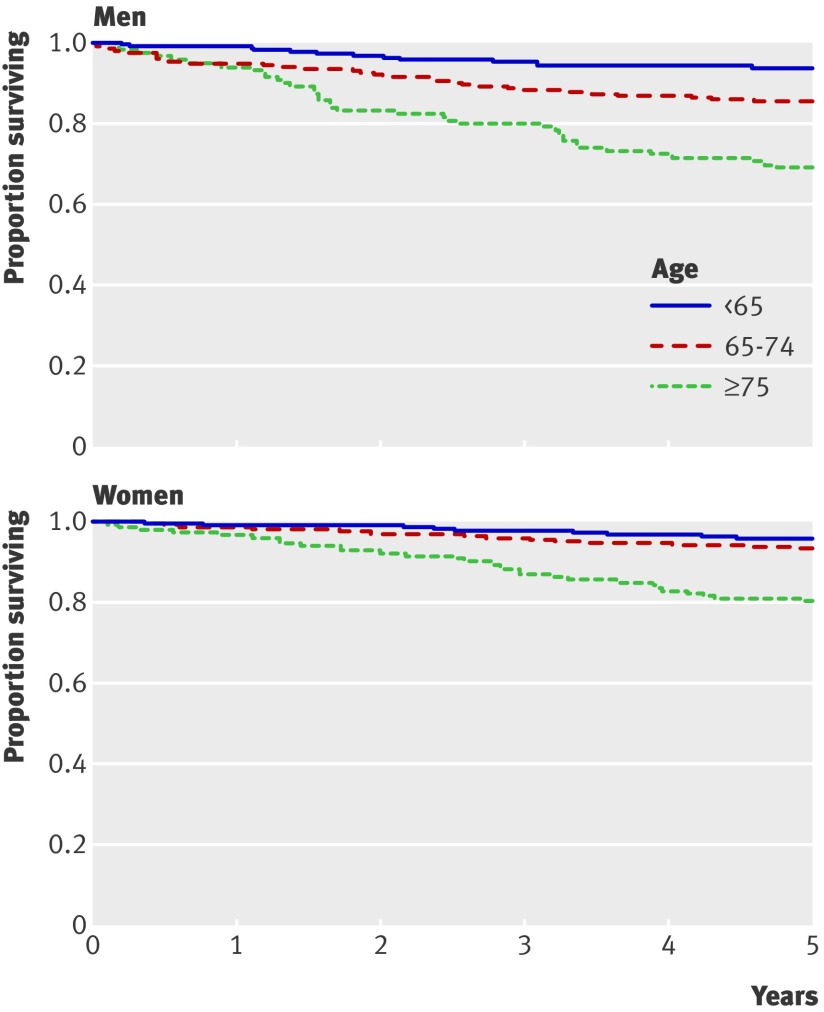
Objective: To ascertain the risk of acute myocardial infarction, invasive cardiac procedures, and mortality among patients with newly diagnosed angina over five years.
Design: Incident cohort study of patients with primary care data linked to secondary care and mortality data.
Setting: 40 primary care practices in Scotland.
Participants: 1785 patients with a diagnosis of angina as their first manifestation of ischaemic heart disease, 1 January 1998 to 31 December 2001.
Main outcome measures: Adjusted hazard ratios for acute myocardial infarction, coronary artery bypass grafting, percutaneous transluminal coronary angioplasty, death from ischaemic heart disease, and all cause mortality, adjusted for demographics, lifestyle risk factors, and comorbidity at cohort entry.
Results: Mean age was 62.3 (SD 11.3). Male sex was associated with an increased risk of acute myocardial infarction (hazard ratio 2.01, 95% confidence interval 1.35 to 2.97), death from ischaemic heart disease (2.80, 1.73 to 4.53), and all cause mortality (1.82, 1.33 to 2.49). Increasing age was associated with acute myocardial infarction (1.04, 1.02 to 1.06, per year of age increase), death from ischaemic heart disease (1.09, 1.06 to 1.11, per year of age increase), and all cause mortality (1.09, 1.07 to 1.11, per year of age increase). Smoking was associated with subsequent acute myocardial infarction (1.94, 1.31 to 2.89), death from ischaemic heart disease (2.12, 1.32 to 3.39), and all cause mortality (2.11, 1.52 to 2.95). Obesity was associated with death from ischaemic heart disease (2.01, 1.17 to 3.45) and all cause mortality (2.20, 1.52 to 3.19). Previous stroke was associated with all cause mortality (1.78, 1.13 to 2.80) and chronic kidney disease with death from ischaemic heart disease (5.72, 1.74 to 18.79). Men were more likely than women to have coronary artery bypass grafting or percutaneous transluminal coronary angioplasty after a diagnosis of angina; older people were less likely to receive percutaneous transluminal coronary angioplasty. Acute myocardial infarction after a diagnosis of angina was associated with an increased risk of death from ischaemic heart disease and all cause mortality (8.84 (5.31 to 14.71) and 4.23 (2.78 to 6.43), respectively). Neither of the invasive cardiac procedures significantly reduced the subsequent risk of all cause mortality.
Conclusions: In this sample of people with incident angina from primary care, there were sex differences in survival and age and sex differences in the provision of revascularisation after a diagnosis. Acute myocardial infarction after a diagnosis of angina was strongly predictive of mortality. To minimise adverse outcomes, optimal preventive treatments should be used in patients with angina.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Sproston K, Primatesta P. Health survey for England 2003. Vol 1. Cardiovascular disease. London: Department of Health, 2003.
-
- Bromley C, Sproston K, Shelton N. The Scottish health survey 2003. Edinburgh: Scottish Executive, 2005.
-
- Buckley B, Murphy AW. Do patients with angina alone have a more benign prognosis than patients with a history of acute myocardial infarction, revascularisation or both? Findings from a community cohort study. Heart 2008;95:461-7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical