

Recombinant tissue plasminogen activator increases blood-brain barrier disruption in acute ischemic stroke: an MR imaging permeability study
- PMID: 19661169
- PMCID: PMC7051295
- DOI: 10.3174/ajnr.A1774
Recombinant tissue plasminogen activator increases blood-brain barrier disruption in acute ischemic stroke: an MR imaging permeability study
Abstract
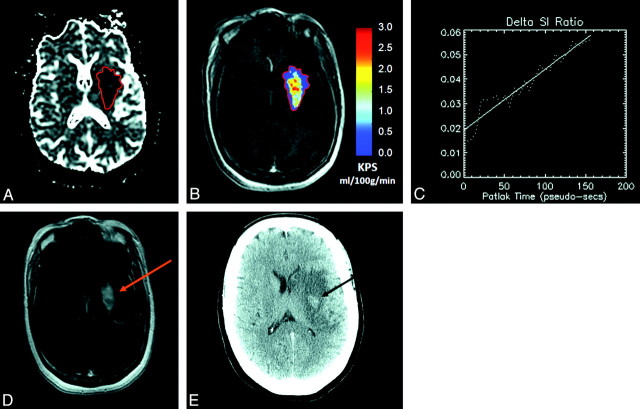
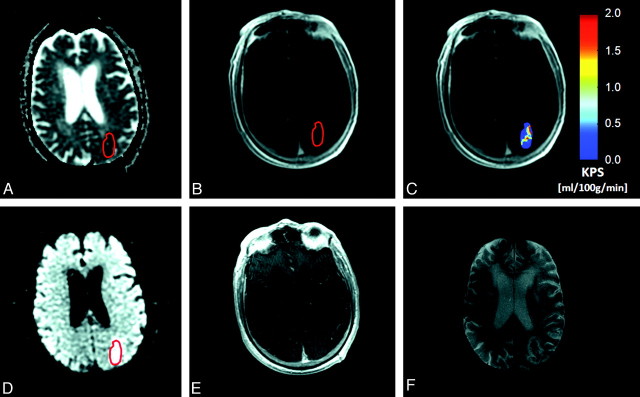
Background and purpose: Although thrombolytic therapy (recombinant tissue plasminogen activator [rtPA]) represents an important step forward in acute ischemic stroke (AIS) management, there is a clear need to identify high-risk patients. The purpose of this study was to investigate the role of quantitative permeability (KPS) MR imaging in patients with AIS treated with and without rtPA. We hypothesized that rtPA would increase KPS and that KPS MR imaging can be used to predict the risk of hemorrhagic transformation (HT).
Materials and methods: Thirty-six patients with AIS were examined within a mean of 3.6 hours of documented symptom onset. KPS MR imaging was performed as part of our AIS protocol. KPS coefficients in the stroke lesion were estimated for all patients, and the relationship between KPS and both HT and rtPA was investigated by using Student t tests. Receiver operating characteristic (ROC) curves were computed for predicting HT from KPS.
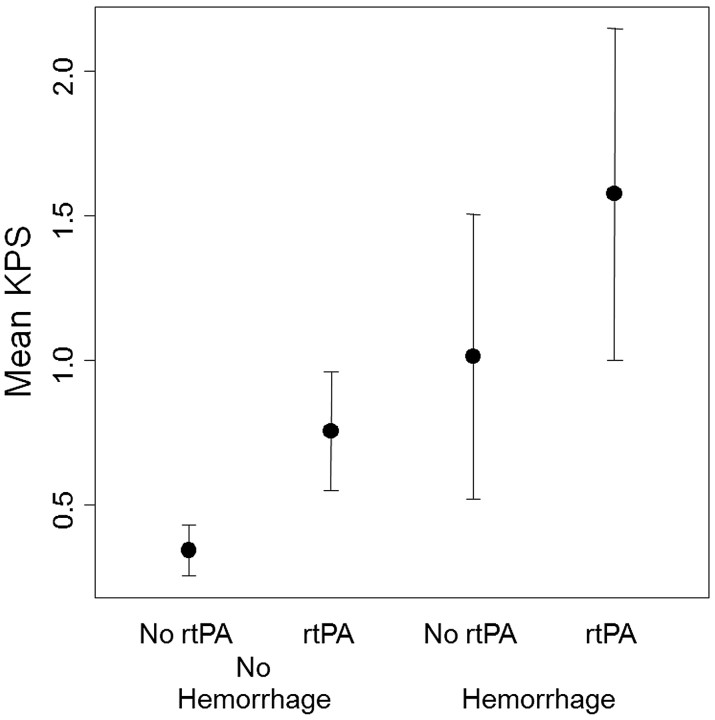
Results: The occurrence rate of HT for patients who received rtPA and those who did not was 43% and 37%, respectively. Assessment of KPS in the lesion revealed significant differences between those who hemorrhaged and those who did not (P < .0001) as well as between rtPA-treated and untreated patients (P = .008). ROC analysis indicated a KPS threshold of 0.67 mL/100 g/min, with a sensitivity of 92% and a specificity of 78%.
Conclusions: The results of this study indicate that KPS is able to identify patients at higher risk of HT and may allow use of physiologic imaging rather than time from onset of symptoms to guide treatment decision.
Figures
References
-
- Smith W, Sung G, Starkman S, et al. Safety and efficacy of mechanical embolectomy in acute ischemic stroke: results of the MERCI trial. Stroke 2005;36:1432–38 - PubMed
-
- Lyden P, Zivin JA. Hemorrhagic transformation after cerebral ischemia: mechanisms and incidence. Cerebrovasc Brain Met Rev 1993;5:1–16 - PubMed
-
- Intracerebral hemorrhage after intravenous t-PA therapy for ischemic stroke: The NINDS tPA Stroke Study Group. Stroke 1997;28:2109–18 - PubMed
-
- Larrue V, von Kummer R, del Zoppo G, et al. Hemorrhagic transformation in acute ischemic stroke: potential contributing factors in the European Cooperative Acute Stroke Study. Stroke 1997;28:957–60 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical