

Hyperglycemia-related mortality in critically ill patients varies with admission diagnosis
- PMID: 19661802
- PMCID: PMC2905804
- DOI: 10.1097/CCM.0b013e3181b083f7
Hyperglycemia-related mortality in critically ill patients varies with admission diagnosis
Abstract
Objectives: Hyperglycemia during critical illness is common and is associated with increased mortality. Intensive insulin therapy has improved outcomes in some, but not all, intervention trials. It is unclear whether the benefits of treatment differ among specific patient populations. The purpose of the study was to determine the association between hyperglycemia and risk- adjusted mortality in critically ill patients and in separate groups stratified by admission diagnosis. A secondary purpose was to determine whether mortality risk from hyperglycemia varies with intensive care unit type, length of stay, or diagnosed diabetes.
Design: Retrospective cohort study.
Setting: One hundred seventy-three U.S. medical, surgical, and cardiac intensive care units.
Patients: Two hundred fifty-nine thousand and forty admissions from October 2002 to September 2005; unadjusted mortality rate, 11.2%.
Interventions: None.
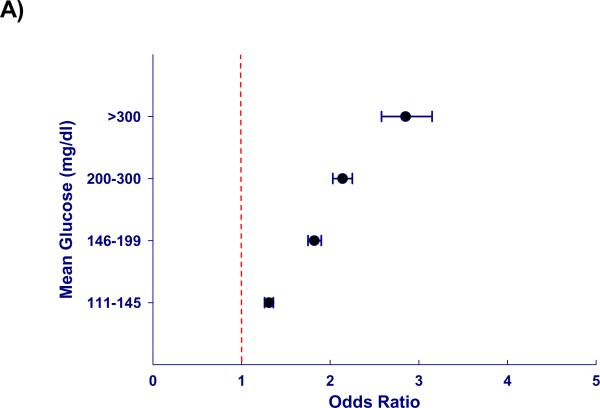
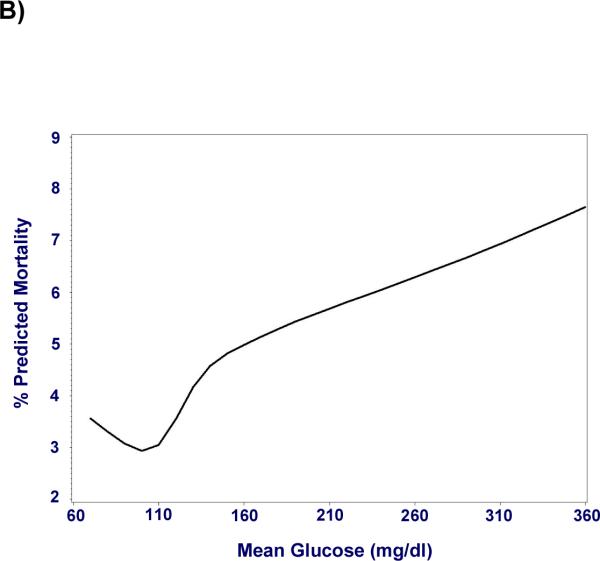
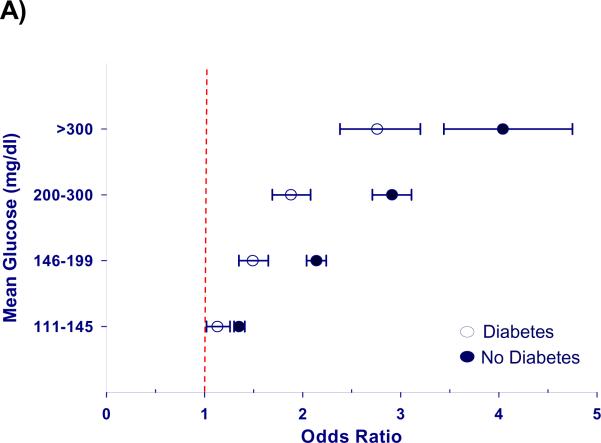
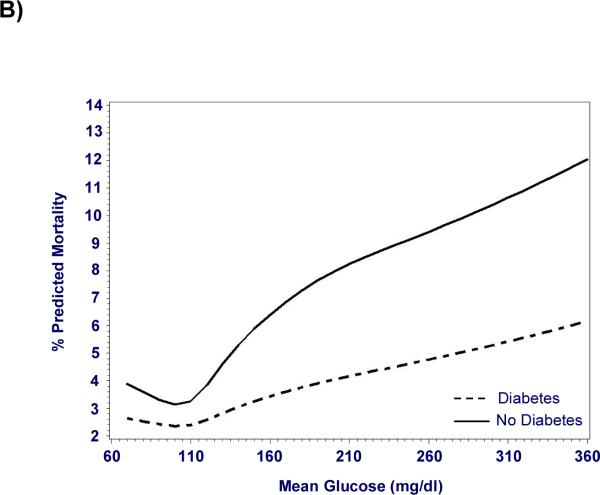
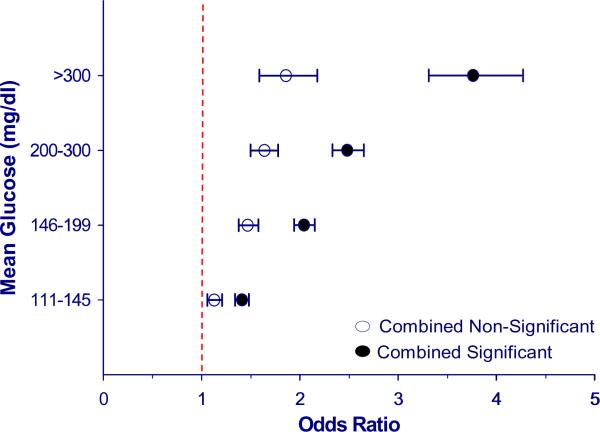
Measurements and main results: A two-level logistic regression model determined the relationship between glycemia and mortality. Age, diagnosis, comorbidities, and laboratory variables were used to calculate a predicted mortality rate, which was then analyzed with mean glucose to determine the association of hyperglycemia with hospital mortality. Hyperglycemia was associated with increased mortality independent of illness severity. Compared with normoglycemic individuals (70-110 mg/dL), adjusted odds of mortality (odds ratio, [95% confidence interval]) for mean glucose 111-145, 146-199, 200-300, and >300 mg/dL was 1.31 (1.26-1.36), 1.82 (1.74-1.90), 2.13 (2.03-2.25), and 2.85 (2.58-3.14), respectively. Furthermore, the adjusted odds of mortality related to hyperglycemia varied with admission diagnosis, demonstrating a clear association in some patients (acute myocardial infarction, arrhythmia, unstable angina, pulmonary embolism) and little or no association in others. Hyperglycemia was associated with increased mortality independent of intensive care unit type, length of stay, and diabetes.
Conclusions: The association between hyperglycemia and mortality implicates hyperglycemia as a potentially harmful and correctable abnormality in critically ill patients. The finding that hyperglycemia-related risk varied with admission diagnosis suggests differences in the interaction between specific medical conditions and injury from hyperglycemia. The design and interpretation of future trials should consider the primary disease states of patients and the balance of medical conditions in the intensive care unit studied.
Figures
Comment in
-
Inpatient hyperglycemia management: the voyage continues!Crit Care Med. 2009 Dec;37(12):3165-6. doi: 10.1097/CCM.0b013e3181b3a958. Crit Care Med. 2009. PMID: 19923934 No abstract available.
-
Hyperglycemia-related mortality in critically ill patients varies with admission diagnosis.Crit Care Med. 2010 May;38(5):1388; author reply 1388-9. doi: 10.1097/CCM.0b013e3181d8a38b. Crit Care Med. 2010. PMID: 20404639 No abstract available.
References
-
- Barsheshet A, Garty M, Grossman E, et al. Admission blood glucose level and mortality among hospitalized nondiabetic patients with heart failure. Arch Intern Med. 2006;166(15):1613–1619. - PubMed
-
- Bochicchio GV, Sung J, Joshi M, et al. Persistent hyperglycemia is predictive of outcome in critically ill trauma patients. J Trauma. 2005;58(5):921–924. - PubMed
-
- Capes SE, Hunt D, Malmberg K, et al. Stress hyperglycaemia and increased risk of death after myocardial infarction in patients with and without diabetes: a systematic overview. Lancet. 2000;355(9206):773–778. - PubMed
-
- Capes SE, Hunt D, Malmberg K, et al. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke. 2001;32(10):2426–2432. - PubMed
-
- Faustino EV, Apkon M. Persistent hyperglycemia in critically ill children. J Pediatr. 2005;146(1):30–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
