

The location of the inferior and superior temporal blood vessels and interindividual variability of the retinal nerve fiber layer thickness
- PMID: 19661824
- PMCID: PMC2889235
- DOI: 10.1097/IJG.0b013e3181af31ec
The location of the inferior and superior temporal blood vessels and interindividual variability of the retinal nerve fiber layer thickness
Abstract
Purpose: To determine if adjusting for blood vessel (BV) location can decrease the intersubject variability of retinal nerve fiber layer (RNFL) thickness measured with optical coherence tomography (OCT).
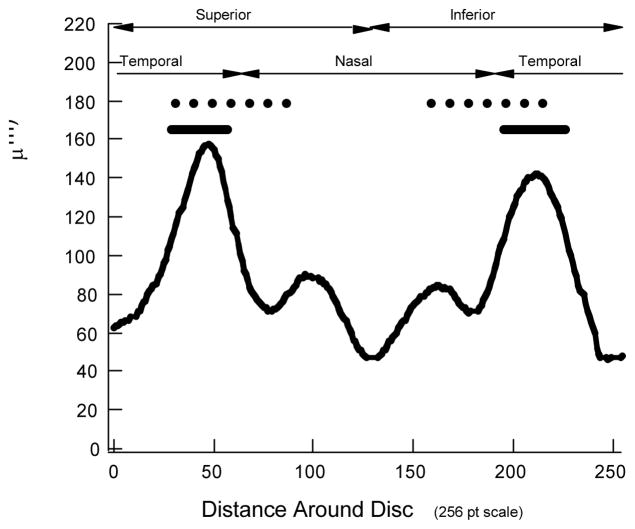
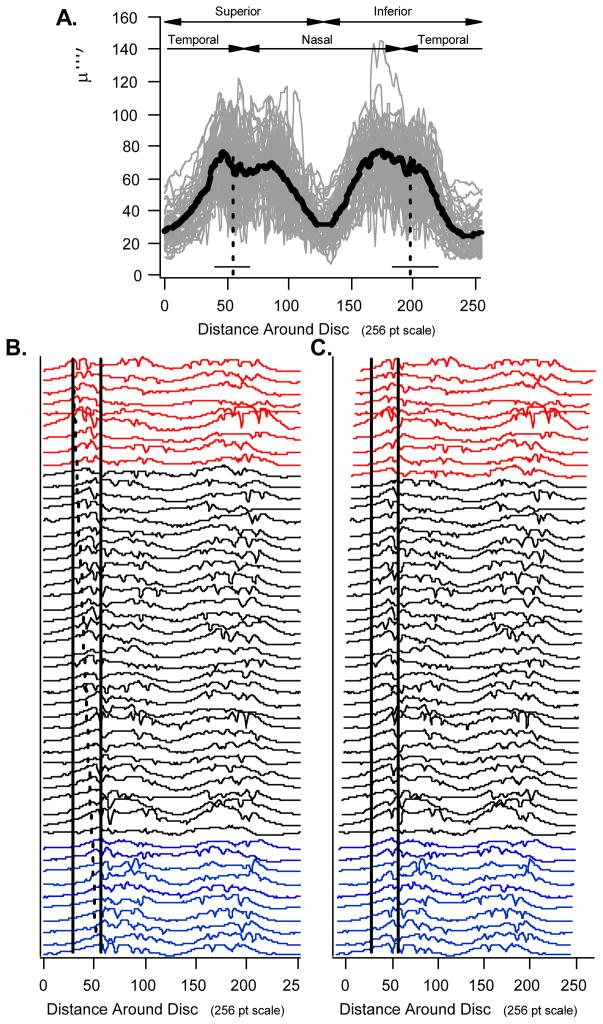
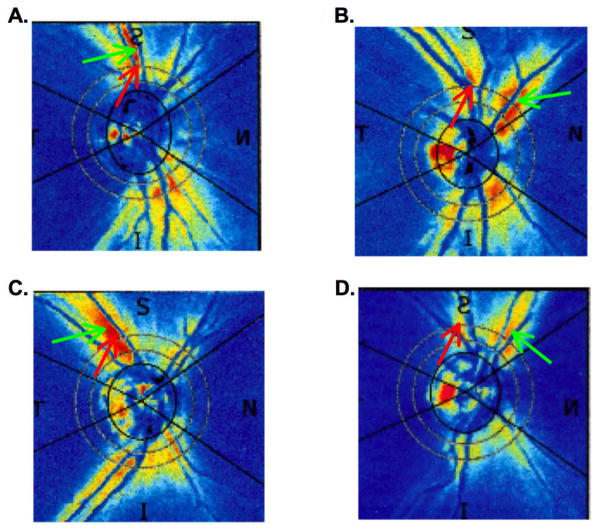
Subjects and methods: One eye of 50 individuals with normal vision was tested with OCT and scanning laser polarimetry (SLP). The SLP and OCT RNFL thickness profiles were determined for a peripapillary circle 3.4 mm in diameter. The midpoints between the superior temporal vein and artery (STva) and the inferior temporal vein and artery (ITva) were determined at the location where the vessels cross the 3.4 mm circle. The average OCT and SLP RNFL thicknesses for quadrants and arcuate sectors of the lower and upper optic disc were obtained before and after adjusting for BV location. This adjustment was carried out by shifting the RNFL profiles based upon the locations of the STva and ITva relative to the mean locations of all 50 individuals.
Results: Blood vessel locations ranged over 39 (STva) and 33 degrees (ITva) for the 50 eyes. The location of the leading edge of the OCT and SLP profiles was correlated with the location of the BVs for both the superior [r=0.72 (OCT) and 0.72 (SLP)] and inferior [r=0.34 and 0.43] temporal vessels. However, the variability in the OCT and SLP thickness measurements showed little change due to shifting. After shifting, the difference in the coefficient of variation ranged from -2.1% (shifted less variable) to +1.7% (unshifted less variable).
Conclusions: The shape of the OCT and SLP RNFL profiles varied systematically with the location of the superior and inferior superior veins and arteries. However, adjusting for the location of these major temporal BVs did not decrease the variability for measures of OCT or SLP RNFL thickness.
Figures






Similar articles
-
Scanning laser polarimetry, but not optical coherence tomography predicts permanent visual field loss in acute nonarteritic anterior ischemic optic neuropathy.Invest Ophthalmol Vis Sci. 2013 Aug 15;54(8):5514-9. doi: 10.1167/iovs.13-12253. Invest Ophthalmol Vis Sci. 2013. PMID: 23838768 Free PMC article.
-
Blood vessel contributions to retinal nerve fiber layer thickness profiles measured with optical coherence tomography.J Glaucoma. 2008 Oct-Nov;17(7):519-28. doi: 10.1097/IJG.0b013e3181629a02. J Glaucoma. 2008. PMID: 18854727 Free PMC article.
-
Retinal imaging by laser polarimetry and optical coherence tomography evidence of axonal degeneration in multiple sclerosis.Arch Neurol. 2008 Jul;65(7):924-8. doi: 10.1001/archneur.65.7.924. Arch Neurol. 2008. PMID: 18625859
-
Retinal Blood Vessel Distribution Correlates With the Peripapillary Retinal Nerve Fiber Layer Thickness Profile as Measured With GDx VCC and ECC.J Glaucoma. 2015 Jun-Jul;24(5):389-95. doi: 10.1097/IJG.0000000000000237. J Glaucoma. 2015. PMID: 25719231 Free PMC article.
-
Does the ISNT Rule Apply to the Retinal Nerve Fiber Layer?J Glaucoma. 2016 Jan;25(1):e1-4. doi: 10.1097/IJG.0000000000000064. J Glaucoma. 2016. PMID: 24777047
Cited by
-
Scanning laser topography and scanning laser polarimetry: comparing both imaging methods at same distances from the optic nerve head.Open Ophthalmol J. 2012;6:6-16. doi: 10.2174/1874364101206010006. Epub 2012 Mar 22. Open Ophthalmol J. 2012. PMID: 22496715 Free PMC article.
-
Artifacts and Anatomic Variations in Optical Coherence Tomography.Turk J Ophthalmol. 2020 Apr 29;50(2):99-106. doi: 10.4274/tjo.galenos.2019.78000. Turk J Ophthalmol. 2020. PMID: 32367701 Free PMC article. Review.
-
Influence of the disc-fovea angle on limits of RNFL variability and glaucoma discrimination.Invest Ophthalmol Vis Sci. 2014 Oct 9;55(11):7332-42. doi: 10.1167/iovs.14-14962. Invest Ophthalmol Vis Sci. 2014. PMID: 25301880 Free PMC article.
-
Optical coherence tomography-measured retinal nerve fiber layer thickness values compensated with a multivariate model and discrimination between stable and progressing glaucoma suspects.Graefes Arch Clin Exp Ophthalmol. 2022 Jan;260(1):225-233. doi: 10.1007/s00417-021-05329-3. Epub 2021 Aug 5. Graefes Arch Clin Exp Ophthalmol. 2022. PMID: 34350469 Free PMC article.
-
Impact of optical coherence tomography scan direction on the reliability of peripapillary retinal nerve fiber layer measurements.PLoS One. 2021 Feb 22;16(2):e0247670. doi: 10.1371/journal.pone.0247670. eCollection 2021. PLoS One. 2021. PMID: 33617580 Free PMC article.
References
-
- Schuman JS, Hee MR, Puliafito CA, et al. Quantification of nerve fiber layer thickness in normal and glaucomatous eyes using optical coherence tomography. Arch Ophthalmol. 1995;113:586–596. - PubMed
-
- Fujimoto JG, Hee MR, Huang D, et al. Principles of optical coherence tomography. In: Schuman JS, editor. Optical Coherence Tomography of Ocular Diseases. Puliafito CA: Fujimoto, JG; Slack Inc; NJ: 2004.
-
- Hee MR, Fujimoto JG, Ko T, et al. Interpretation of the optical coherence tomography image. In: Schuman JS, editor. Optical Coherence Tomography of Ocular Diseases. Puliafito CA: Fujimoto, JG; Slack Inc; NJ: 2004.
-
- Brusini P, Salvetat ML, Zeppieri M, et al. Comparison between GDx VCC scanning laser polarimetry and Stratus OCT optical coherence tomography in the diagnosis of chronic glaucoma. Acta Ophthalmol Scand. 2006;84:650–655. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
