

Brain structure and obesity
- PMID: 19662657
- PMCID: PMC2826530
- DOI: 10.1002/hbm.20870
Brain structure and obesity
Abstract
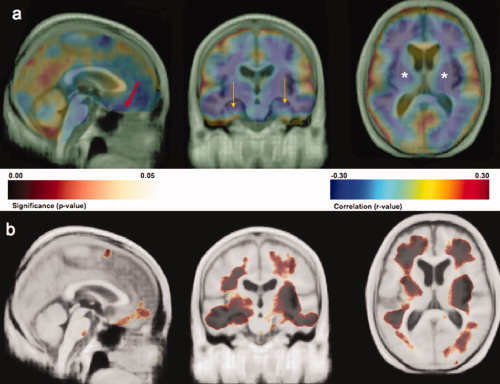
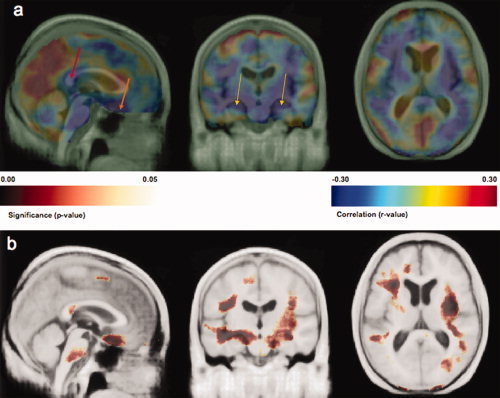
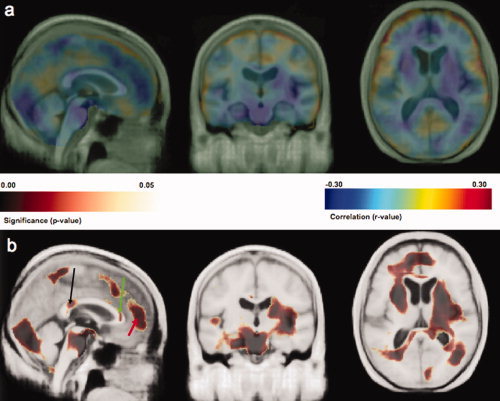
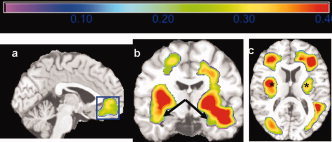
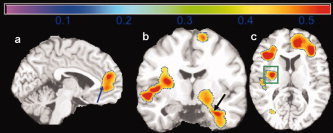
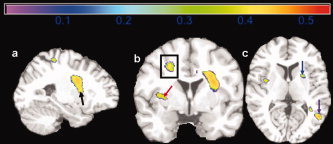
Obesity is associated with increased risk for cardiovascular health problems including diabetes, hypertension, and stroke. These cardiovascular afflictions increase risk for cognitive decline and dementia, but it is unknown whether these factors, specifically obesity and Type II diabetes, are associated with specific patterns of brain atrophy. We used tensor-based morphometry (TBM) to examine gray matter (GM) and white matter (WM) volume differences in 94 elderly subjects who remained cognitively normal for at least 5 years after their scan. Bivariate analyses with corrections for multiple comparisons strongly linked body mass index (BMI), fasting plasma insulin (FPI) levels, and Type II Diabetes Mellitus (DM2) with atrophy in frontal, temporal, and subcortical brain regions. A multiple regression model, also correcting for multiple comparisons, revealed that BMI was still negatively correlated with brain atrophy (FDR <5%), while DM2 and FPI were no longer associated with any volume differences. In an Analysis of Covariance (ANCOVA) model controlling for age, gender, and race, obese subjects with a high BMI (BMI > 30) showed atrophy in the frontal lobes, anterior cingulate gyrus, hippocampus, and thalamus compared with individuals with a normal BMI (18.5-25). Overweight subjects (BMI: 25-30) had atrophy in the basal ganglia and corona radiata of the WM. Overall brain volume did not differ between overweight and obese persons. Higher BMI was associated with lower brain volumes in overweight and obese elderly subjects. Obesity is therefore associated with detectable brain volume deficits in cognitively normal elderly subjects.
2009 Wiley-Liss, Inc.
Figures
References
-
- Apostolova LG, Dutton RA, Dinov ID, Hayashi KM, Toga AW, Cummings JL, Thompson PM ( 2006): Conversion of mild cognitive impairment to Alzheimer disease predicted by hippocampal atrophy maps. Arch Neurol 63: 693–699. - PubMed
-
- Arvanitakis Z, Schneider JA, Wilson RS, Li Y, Arnold SE, Wang Z, Bennett DA ( 2006): Diabetes is related to cerebral infarction but not to AD pathology in older persons. Neurology 67: 1960–1965. - PubMed
-
- Ashburner J, Friston KJ ( 2000): Voxel‐based morphometry—The methods. Neuroimage 11: 805–821. - PubMed
-
- Bian L, Yang JD, Guo TW, Sun Y, Duan SW, Chen WY, Pan YX, Yeng GY, He L ( 2004): Insulin‐degrading enzyme and Alzheimer disease. Neurology 63: 241–245. - PubMed
-
- Braak H, Braak E ( 1991): Neuropathological stageing of Alzheimer‐related changes. Acta Neuropathol 82: 239–259. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R21 EB001561/EB/NIBIB NIH HHS/United States
- AG15928/AG/NIA NIH HHS/United States
- AG016570/AG/NIA NIH HHS/United States
- R01 AG015928/AG/NIA NIH HHS/United States
- R21 RR019771/RR/NCRR NIH HHS/United States
- R56 AG020098/AG/NIA NIH HHS/United States
- EB01651/EB/NIBIB NIH HHS/United States
- AG05133/AG/NIA NIH HHS/United States
- AG 20098/AG/NIA NIH HHS/United States
- P50 AG005133/AG/NIA NIH HHS/United States
- R01 AG020098/AG/NIA NIH HHS/United States
- RR019771/RR/NCRR NIH HHS/United States
- P50 AG016570/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
