

High-dose daclizumab for the treatment of juvenile idiopathic arthritis-associated active anterior uveitis
- PMID: 19664754
- PMCID: PMC2922905
- DOI: 10.1016/j.ajo.2009.06.003
High-dose daclizumab for the treatment of juvenile idiopathic arthritis-associated active anterior uveitis
Abstract
Purpose: To provide preliminary data regarding the safety and efficacy of high-dose intravenous daclizumab (Zenapax; Roche Inc, Nutley, New Jersey, USA) therapy for the treatment of juvenile idiopathic arthritis (JIA)-associated active anterior uveitis.
Design: Interventional case series; open-label prospective, phase II pilot study.
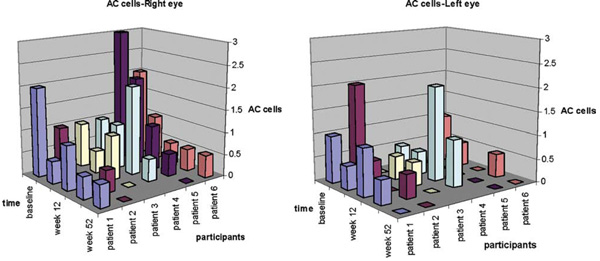
Methods: Six patients were recruited into the study and received daclizumab therapy at doses of 8 mg/kg at baseline, 4 mg/kg at week 2, and 2 mg/kg every 4 weeks thereafter, for a total of 52 weeks. The study was done at the National Eye Institute between June 29, 2005 and July 9, 2008. The primary outcome was a two-step decrease in inflammation grade assessed at week 12. Primary safety outcome was assessed at weeks 2 and 4. The ocular inflammation was assessed according to the Standardization of Uveitis Nomenclature criteria.
Results: Four of the 6 participants achieved two-step reduction in anterior chamber cells according to Standardization of Uveitis Nomenclature Working Group grading scheme for anterior chamber cells 12 weeks into the study and met the primary efficacy endpoint. One additional patient responded to reinduction whereas 1 patient failed reinduction and was considered an ocular treatment failure. Visual acuity improved from a mean of 68 Early Treatment Diabetic Retinopathy Study letters in the worse eye to a mean of 79.6 letters (2 Snellen lines). Three participants were terminated before 52 weeks: First, because of a rash possibly induced by daclizumab; Second, because of ocular treatment failure; and Last, because of uncontrolled systemic manifestations of JIA.
Conclusion: High-dose intravenous daclizumab can help reduce active inflammation in active JIA-associated anterior uveitis; however, patients need to be monitored for potential side effects. Larger randomized trials are needed to better assess treatment effect and safety.
Trial registration: ClinicalTrials.gov NCT00130637.
Conflict of interest statement
The authors indicate no financial conflict of interest.
Figures
References
-
- Petty RE, Southwood TR, Manners P, et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31:390–392. - PubMed
-
- Ravelli A, Felici E, Magni-Manzoni S, et al. Patients with anti-nuclear antibody-positive juvenile idiopathic arthritis constitute a homogeneous subgroup irrespective of the course of joint disease. Arthritis Rheum. 2005;52:826–832. - PubMed
-
- Kotaniemi K, Kautiainen H, Karma A, Aho K. Occurrence of uveitis in recently diagnosed juvenile chronic arthritis: a prospective study. Ophthalmology. 2001;108:2071–2075. - PubMed
-
- Foster CS. Diagnosis and treatment of juvenile idiopathic arthritis-associated uveitis. Curr Opin Ophthalmol. 2003;14:395–398. - PubMed
-
- Chalom EC, Goldsmith DP, Koehler MA, et al. Prevalence and outcome of uveitis in a regional cohort of patients with juvenile rheumatoid arthritis. J Rheumatol. 1997;24:2031–2034. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
