

The supplementary motor area contributes to the timing of the anticipatory postural adjustment during step initiation in participants with and without Parkinson's disease
- PMID: 19665521
- PMCID: PMC2762010
- DOI: 10.1016/j.neuroscience.2009.08.002
The supplementary motor area contributes to the timing of the anticipatory postural adjustment during step initiation in participants with and without Parkinson's disease
Abstract
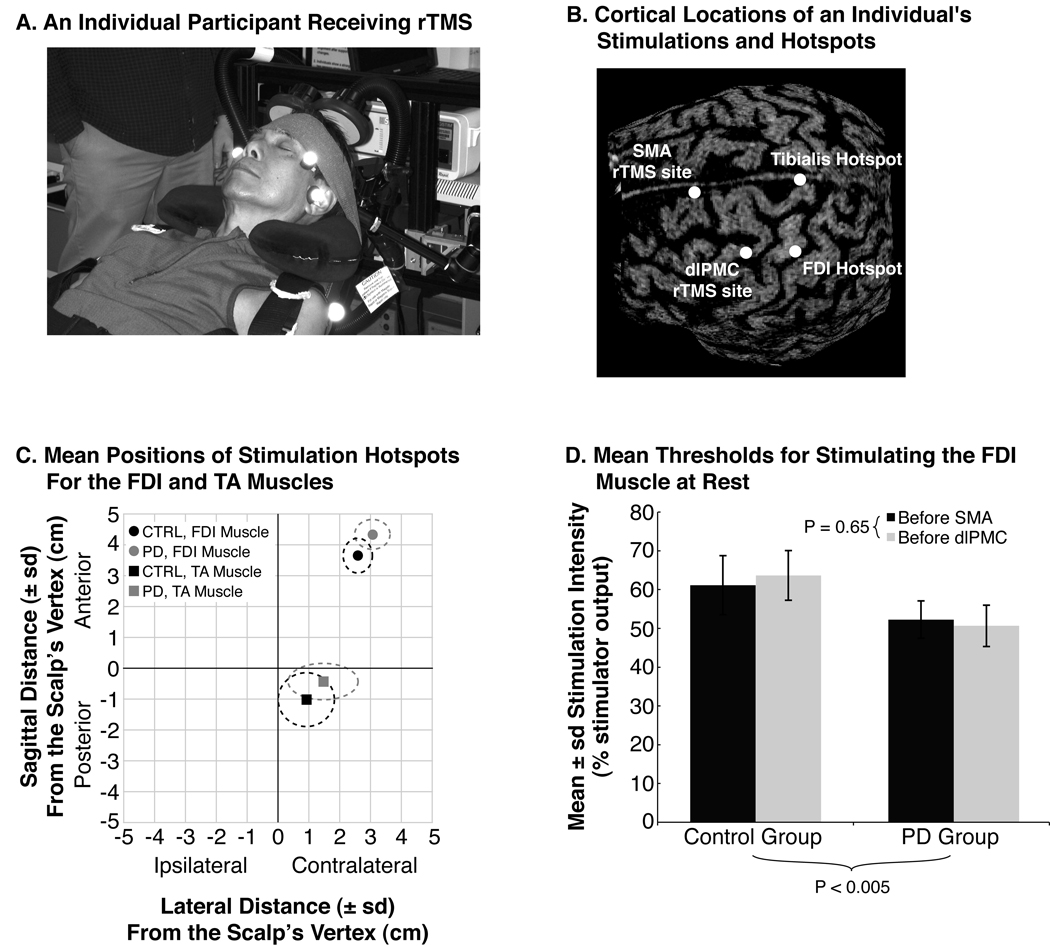
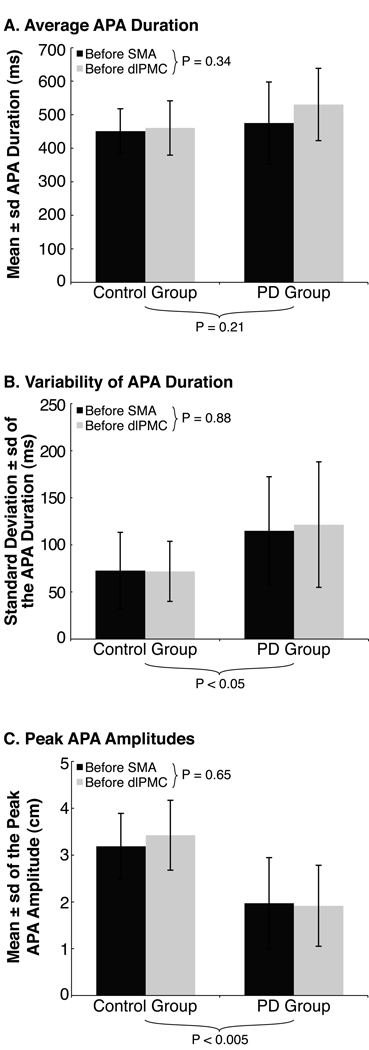
The supplementary motor area (SMA) is thought to contribute to the generation of anticipatory postural adjustments (APAs, which act to stabilize supporting body segments prior to movement), but its precise role remains unclear. In addition, participants with Parkinson's disease (PD) exhibit impaired function of the SMA as well as decreased amplitudes and altered timing of the APA during step initiation, but the contribution of the SMA to these impairments also remains unclear. To determine how the SMA contributes to generating the APA and to the impaired APAs of participants with PD, we examined the voluntary steps of eight participants with PD and eight participants without PD, before and after disrupting the SMA and dorsolateral premotor cortex (dlPMC), in separate sessions, with 1-Hz repetitive transcranial magnetic stimulation (rTMS). Both groups exhibited decreased durations of their APAs after rTMS over the SMA but not over the dlPMC. Peak amplitudes of the APAs were unaffected by rTMS to either site. The symptom severity of the participants with PD positively correlated with the extent that rTMS over the SMA affected the durations of their APAs. The results suggest that the SMA contributes to the timing of the APA and that participants with PD exhibit impaired timing of their APAs, in part, due to progressive dysfunction of circuits associated with the SMA.
Figures


References
-
- Bestmann S, Baudewig J, Siebner HR, Rothwell JC, Frahm J. BOLD MRI responses to repetitive TMS over human dorsal premotor cortex. Neuroimage. 2005;28:22–29. - PubMed
-
- Bloem BR, Grimbergen YA, Cramer M, Willemsen M, Zwinderman AH. Prospective assessment of falls in Parkinson’s disease. J Neurol. 2001;248:950–958. - PubMed
-
- Bloem BR, Hausdorff JM, Visser JE, Giladi N. Falls and freezing of gait in Parkinson’s disease: a review of two interconnected, episodic phenomena. Mov Disord. 2004;19:871–884. - PubMed
-
- Boylan LS, Pullman SL, Lisanby SH, Spicknall KE, Sackeim HA. Repetitive transcranial magnetic stimulation to SMA worsens complex movements in Parkinson’s disease. Clin Neurophysiol. 2001;112:259–264. - PubMed
-
- Braak H, Del Tredici K, Bratzke H, Hamm-Clement J, Sandmann-Keil D, Rüb U. Staging of the intracerebral inclusion body pathology associated with idiopathic Parkinson’s disease (preclinical and clinical stages) J Neurol. 2002;249 Suppl 3:1–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
