

Identification, molecular characterization, clinical prognosis, and therapeutic targeting of human bladder tumor-initiating cells
- PMID: 19666525
- PMCID: PMC2720852
- DOI: 10.1073/pnas.0906549106
Identification, molecular characterization, clinical prognosis, and therapeutic targeting of human bladder tumor-initiating cells
Abstract
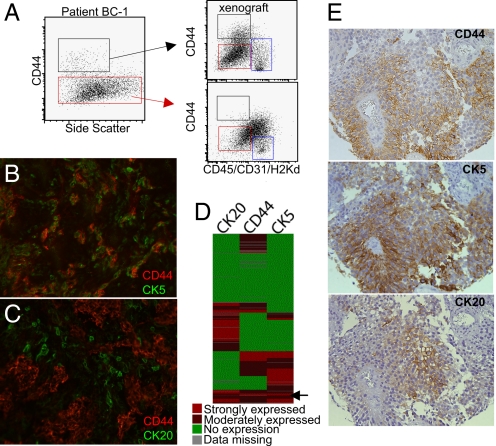
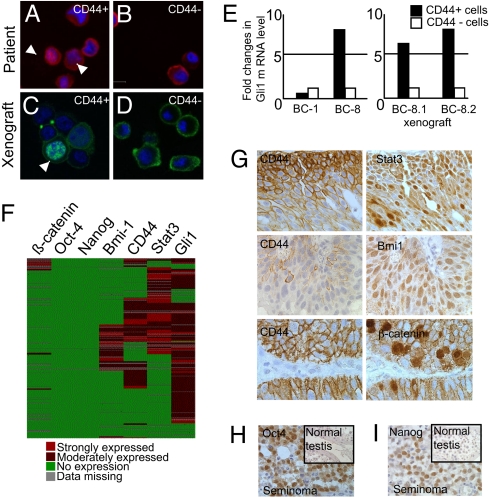
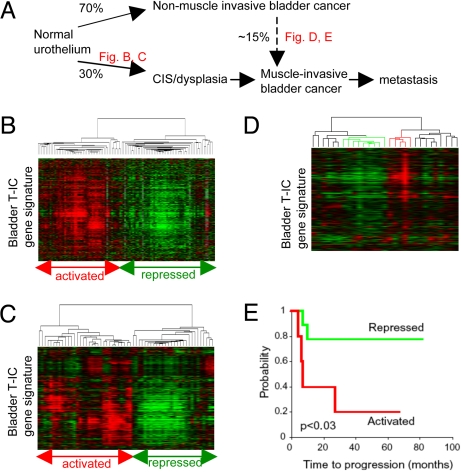
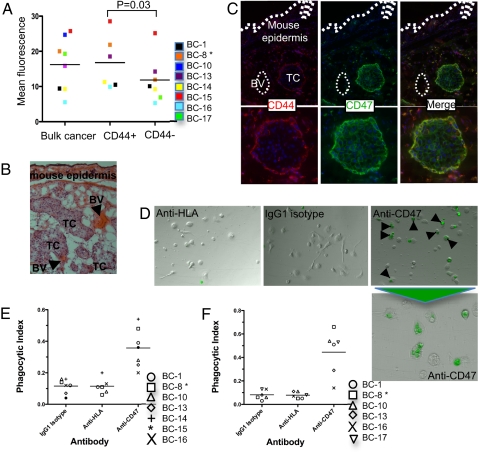
Major clinical issues in bladder cancer include the identification of prediction markers and novel therapeutic targets for invasive bladder cancer. In the current study, we describe the isolation and characterization of a tumor-initiating cell (T-IC) subpopulation in primary human bladder cancer, based on the expression of markers similar to that of normal bladder basal cells (Lineage-CD44(+)CK5(+)CK20(-)). The bladder T-IC subpopulation was defined functionally by its enriched ability to induce xenograft tumors in vivo that recapitulated the heterogeneity of the original tumor. Further, molecular analysis of more than 300 bladder cancer specimens revealed heterogeneity among activated oncogenic pathways in T-IC (e.g., 80% Gli1, 45% Stat3, 10% Bmi-1, and 5% beta-catenin). Despite this molecular heterogeneity, we identified a unique bladder T-IC gene signature by gene chip analysis. This T-IC gene signature, which effectively distinguishes muscle-invasive bladder cancer with worse clinical prognosis from non-muscle-invasive (superficial) cancer, has significant clinical value. It also can predict the progression of a subset of recurring non-muscle-invasive cancers. Finally, we found that CD47, a protein that provides an inhibitory signal for macrophage phagocytosis, is highly expressed in bladder T-ICs compared with the rest of the tumor. Blockade of CD47 by a mAb resulted in macrophage engulfment of bladder cancer cells in vitro. In summary, we have identified a T-IC subpopulation with potential prognostic and therapeutic value for invasive bladder cancer.
Conflict of interest statement
Conflict of interest statement: I.L.W. was a member of the scientific advisory board of Amgen and owns significant Amgen stock; he cofounded and consulted for Systemix; he is a cofounder and director of Stem Cells, Inc.; and he recently cofounded Cellerant, Inc.
Figures
Similar articles
-
Predicting outcomes in non-muscle invasive (Ta/T1) bladder cancer: the role of molecular grade based on luminal/basal phenotype.Virchows Arch. 2019 Oct;475(4):445-455. doi: 10.1007/s00428-019-02593-x. Epub 2019 Jun 25. Virchows Arch. 2019. PMID: 31240474
-
Immunohistochemistry of cytokeratin (CK) 5/6, CD44 and CK20 as prognostic biomarkers of non-muscle-invasive papillary upper tract urothelial carcinoma.Histopathology. 2019 Feb;74(3):483-493. doi: 10.1111/his.13763. Epub 2018 Dec 2. Histopathology. 2019. PMID: 30286252
-
Clinical significance of CD44 variant 9 expression as a prognostic indicator in bladder cancer.Oncol Rep. 2016 Nov;36(5):2852-2860. doi: 10.3892/or.2016.5061. Epub 2016 Sep 1. Oncol Rep. 2016. PMID: 27599396
-
Therapeutic opportunities in the intrinsic subtypes of muscle-invasive bladder cancer.Hematol Oncol Clin North Am. 2015 Apr;29(2):377-94, x-xi. doi: 10.1016/j.hoc.2014.11.003. Hematol Oncol Clin North Am. 2015. PMID: 25836941 Review.
-
Molecular pathways of urothelial development and bladder tumorigenesis.Urol Oncol. 2010 Jul-Aug;28(4):401-8. doi: 10.1016/j.urolonc.2009.04.019. Urol Oncol. 2010. PMID: 20610278 Review.
Cited by
-
Characterization of the stem cell landscape and identification of a stemness-associated prognostic signature in bladder cancer.Cancer Cell Int. 2024 Aug 24;24(1):299. doi: 10.1186/s12935-024-03465-4. Cancer Cell Int. 2024. PMID: 39182054 Free PMC article.
-
Synergy of Histone-Deacetylase Inhibitor AR-42 with Cisplatin in Bladder Cancer.J Urol. 2015 Aug;194(2):547-55. doi: 10.1016/j.juro.2015.02.2918. Epub 2015 Mar 3. J Urol. 2015. PMID: 25748177 Free PMC article.
-
Tumor-Initiating Cells: Emerging Biophysical Methods of Isolation.Curr Stem Cell Rep. 2016 Mar 1;2(1):21-32. doi: 10.1007/s40778-016-0036-6. Epub 2016 Feb 9. Curr Stem Cell Rep. 2016. PMID: 27141429 Free PMC article.
-
p63 expression defines a lethal subset of muscle-invasive bladder cancers.PLoS One. 2012;7(1):e30206. doi: 10.1371/journal.pone.0030206. Epub 2012 Jan 10. PLoS One. 2012. PMID: 22253920 Free PMC article.
-
Cell surface markers of cancer stem cells: diagnostic macromolecules and targets for drug delivery.Drug Deliv Transl Res. 2013 Apr;3(2):121-42. doi: 10.1007/s13346-012-0075-1. Drug Deliv Transl Res. 2013. PMID: 25787981
References
-
- Heppner GH. Tumor heterogeneity. Cancer Res. 1984;44:2259–2265. - PubMed
-
- Kirkels WJ, Pelgrim OE, Debruyne FM, Vooijs GP, Herman CJ. Soft agar culture of human transitional cell carcinoma colonies from urine. Am J Clin Pathol. 1982;78:690–694. - PubMed
-
- Lipponen PK, Eskelinen MJ. Cell proliferation of transitional cell bladder cancer determined by PCNA/cyclin immunostaining. A histopathological description. Anticancer Res. 1992;12:577–583. - PubMed
-
- Reya T, Morrison SJ, Clarke MF, Weissman IL. Stem cells, cancer, and cancer stem cells. Nature. 2001;414:105–111. - PubMed
-
- Polyak K, Hahn WC. Roots and stems: Stem cells in cancer. Nat Med. 2006;12:296–300. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
