

Growth differentiation factor-15 predicts mortality and morbidity after cardiac resynchronization therapy
- PMID: 19666898
- PMCID: PMC2777028
- DOI: 10.1093/eurheartj/ehp300
Growth differentiation factor-15 predicts mortality and morbidity after cardiac resynchronization therapy
Abstract
Aims: The aim of this study was to determine whether growth differentiation factor-15 (GDF-15) predicts mortality and morbidity after cardiac resynchronization therapy (CRT). Growth differentiation factor-15, a transforming growth factor-beta-related cytokine which is up-regulated in cardiomyocytes via multiple stress pathways, predicts mortality in patients with heart failure treated pharmacologically.
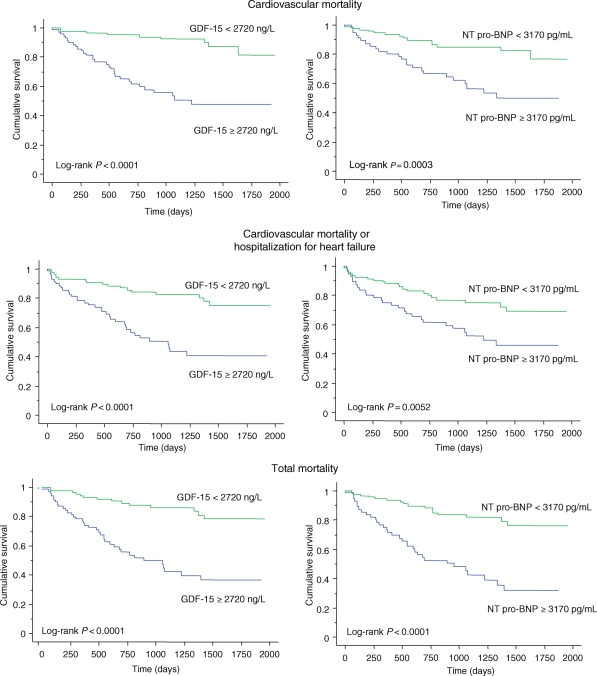
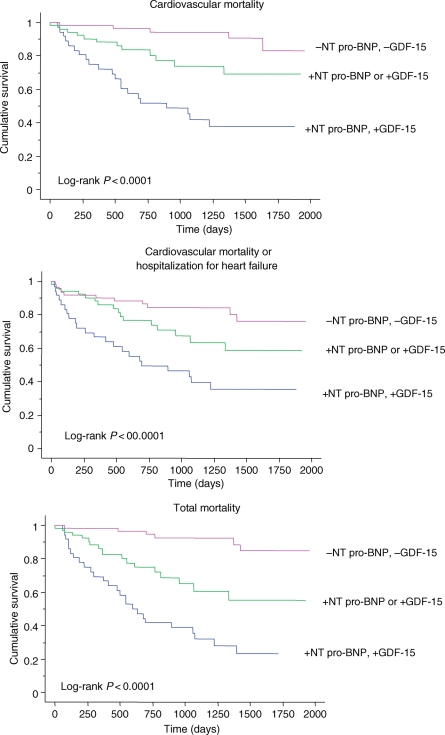
Methods and results: Growth differentiation factor-15 was measured before and 360 days (median) after implantation in 158 patients with heart failure [age 68 +/- 11 years (mean +/- SD), left ventricular ejection fraction (LVEF) 23.1 +/- 9.8%, New York Class Association (NYHA) class III (n = 117) or IV (n = 41), and QRS 153.9 +/- 28.2 ms] undergoing CRT and followed up for a maximum of 5.4 years for events. In a stepwise Cox proportional hazards model with bootstrapping, adopting log GDF-15, log NT pro-BNP, LVEF, and NYHA class as independent variables, only log GDF-15 [hazard ratio (HR), 3.76; P = 0.0049] and log NT pro-BNP (HR, 2.12; P = 0.0171) remained in the final model. In the latter, the bias-corrected slope was 0.85, the optimism (O) was -0.06, and the c-statistic was 0.74, indicating excellent internal validity. In univariate analyses, log GDF-15 [HR, 5.31; 95% confidence interval (CI), 2.31-11.9; likelihood ratio (LR) chi(2) = 14.6; P < 0.0001], NT pro-BNP (HR, 2.79; 95% CI, 1.55-5.26; LR chi(2) = 10.4; P = 0.0004), and the combination of both biomarkers (HR, 7.03; 95% CI, 2.91-17.5; LR chi(2) = 19.1; P < 0.0001) emerged as significant predictors. The biomarker combination was associated with the highest LR chi(2) for all endpoints.
Conclusion: Pre-implant GDF-15 is a strong predictor of mortality and morbidity after CRT, independent of NT pro-BNP. The predictive value of these analytes is enhanced by combined measurement.
Figures
References
-
- Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass D, De Marco T, Carson P, DiCarlo L, DeMets D, White BG, DeVries DW, Feldman AM for the Comparison of Medical Therapy, Pacing and Defibrillation in Heart Failure (COMPANION) Investigators. Cardiac resynchronization therapy with or without an implantable defibrillator in advanced heart failure. N Engl J Med. 2004;350:2140–2150. - PubMed
-
- Cleland JGF, Daubert J-C, Erdmann E, Freemantle N, Gras D, Kappenberger L, Tavazzi L for the Cardiac Resynchronization-Heart Failure (CARE-HF) study investigators. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352:1539–1549. - PubMed
-
- Bax JJ, Abraham T, Barold SS, Breithardt OA, Fung JWH, Garrigue S, Gorcsan J, III, Hayes DL, Kass DA, Knuuti J, Leclercq C, Linde C, Mark DB, Monaghan MJ, Nihoyannopoulos P, Schalij MJ, Stellbrink C, Yu C-M. Cardiac resynchronization therapy: part 1—issues before device implantation. J Am Coll Cardiol. 2005;46:2153–2167. - PubMed
-
- Chung E, Leon A, Tavazzi L, Sun J, Nihoyannopoulos P, Merlino J, Abraham W, Guio S, Leclerq C, Bax J, Yu C-M, Gorcsan J, III, Sutton M, De Sutter J, Murillo J. Results of the Predictors of Response to CRT (PROSPECT) Trial. Circulation. 2008;117:2608–2616. - PubMed
-
- Maisel A. Biomarkers in heart failure. Does prognostic utility translate to clinical futility? J Am Coll Cardiol. 2007;50:1061–1063. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
