

Modern approaches to pediatric brain injury therapy
- PMID: 19667844
- PMCID: PMC2874892
- DOI: 10.1097/TA.0b013e3181ad323a
Modern approaches to pediatric brain injury therapy
Abstract
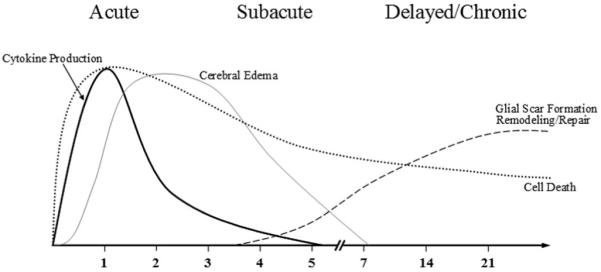
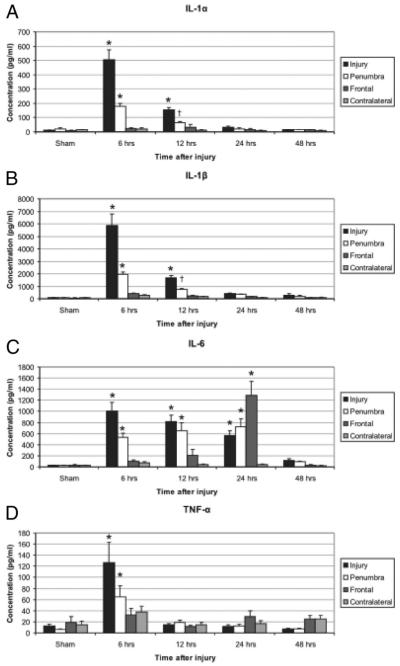
Each year, pediatric traumatic brain injury (TBI) accounts for 435,000 emergency department visits, 37,000 hospital admissions, and approximately 2,500 deaths in the United States. TBI results in immediate injury from direct mechanical force and shear. Secondary injury results from the release of biochemical or inflammatory factors that alter the loco-regional milieu in the acute, subacute, and delayed intervals after a mechanical insult. Preliminary preclinical and clinical research is underway to evaluate the benefit from progenitor cell therapeutics, hypertonic saline infusion, and controlled hypothermia. However, all phase III clinical trials investigating pharmacologic monotherapy for TBI have shown no benefit. A recent National Institutes of Health consensus statement recommends research into multimodality treatments for TBI. This article will review the complex pathophysiology of TBI as well as the possible therapeutic mechanisms of progenitor cell transplantation, hypertonic saline infusion, and controlled hypothermia for possible utilization in multimodality clinical trials.
Figures
References
-
- Langlois JA, Rutland-Brown W, Thomas KE. The incidence of trau-matic brain injury among children in the United States: differences by race. J Head Trauma Rehabil. 2005;20:229–238. - PubMed
-
- McCarthy ML, Serpi T, Kufera JA, Demeter LA, Paidas C. Factors influencing admission among children with a traumatic brain injury. Acad Emerg Med. 2002;9:684–693. - PubMed
-
- Gray DS, Burnham RS. Preliminary outcome analysis of a long-term rehabilitation program for severe acquired brain injury. Arch Phys Med Rehabil. 2000;81:1447–1456. - PubMed
-
- Cowen TD, Meythaler JM, DeVivo MJ, Ivie CS, III, Lebow J, Novack TA. Influence of early variables in traumatic brain injury on functional independence measure scores and rehabilitation length of stay and charges. Arch Phys Med Rehabil. 1995;76:797–803. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
