

Lower eyelid lengthening surgery targeting the posterior layer of the lower eyelid retractors via a transcutaneous approach
- PMID: 19668503
- PMCID: PMC2704509
Lower eyelid lengthening surgery targeting the posterior layer of the lower eyelid retractors via a transcutaneous approach
Abstract
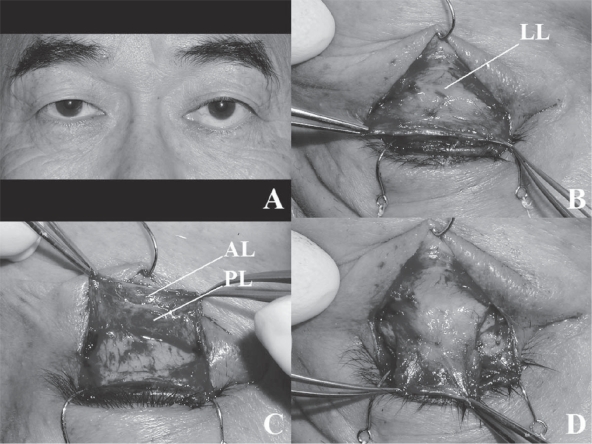
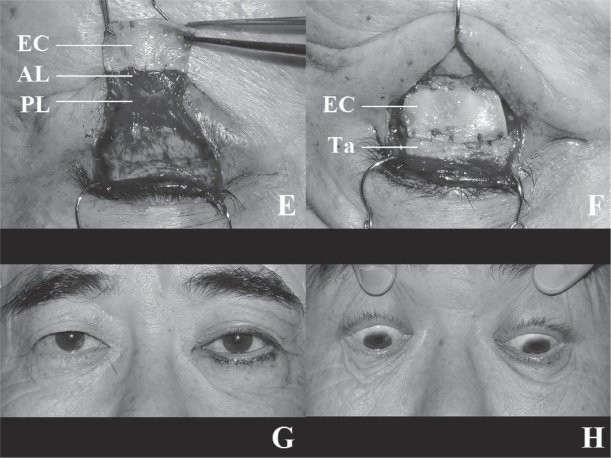
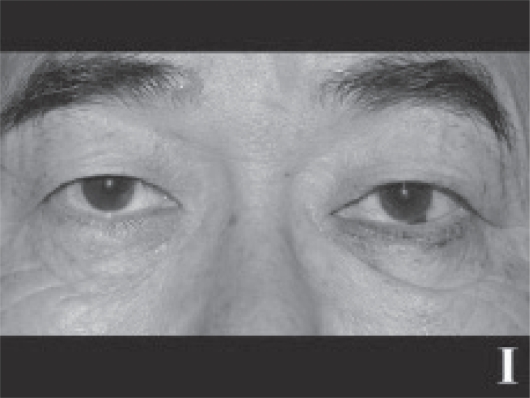
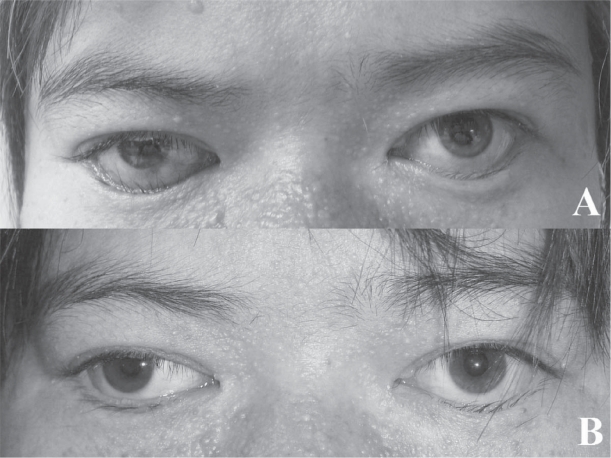
The lower eyelid retractors consist of double layers, the posterior layer of which is the main tractional component. Therefore, shortening of the posterior layer of the lower eyelid retractors causes lower eyelid retraction or cicatricial entropion. Based on this concept, we report a modified lower eyelid lengthening surgery involving complete recession of the posterior layer of the lower eyelid retractors by way of a transcutaneous approach that leaves the palpebral conjunctiva intact and inserts ear cartilage as a rigid spacer between the lower edge of the tarsal plate and the recessed anterior layer of the lower eyelid retractors. This procedure completely extirpated the preoperative maladjusted states of lower eyelid retraction and cicatricial entropion. Our procedure also prevented postoperative discomfort of the ocular surface due to the intact palpebral conjunctiva. As well, lower eyelid mobility and contour were good and within their respective permissible ranges. The lower eyelid lengthening surgery focusing on the posterior layer of the lower eyelid retractors using auricular cartilage via a transcutaneous approach is a useful procedure for lower eyelid retraction or cicatricial entropion.
Keywords: cicatricial entropion; ear cartilage; lower eyelid retraction; posterior layer of the lower eyelid retractors; transcutaneous approach.
Figures
Similar articles
-
Correction of Cicatricial Lower Eyelid Retraction and Entropion With Combined Scar Release, Hard Palate Graft, and Lateral Canthal Suspension.J Craniofac Surg. 2024 Mar-Apr 01;35(2):622-625. doi: 10.1097/SCS.0000000000009798. Epub 2023 Nov 6. J Craniofac Surg. 2024. PMID: 37934969
-
CASE REPORT How to Repair the Lower Eyelid Retraction, Resulting From the Primary Surgery for Epiblepharon?Eplasty. 2013 Oct 31;13:e55. eCollection 2013. Eplasty. 2013. PMID: 24324846 Free PMC article.
-
A conjunctival-sparing surgical technique for lower eyelid cicatricial entropion repair in ocular cicatricial pemphigoid.Orbit. 2020 Feb;39(1):23-30. doi: 10.1080/01676830.2019.1573434. Epub 2019 Feb 7. Orbit. 2020. PMID: 30732510
-
Eyelid malposition: lower lid entropion and ectropion.Medicina (Kaunas). 2006;42(11):881-4. Medicina (Kaunas). 2006. PMID: 17172788 Review.
-
Eyelid entropion.Semin Ophthalmol. 2010 May;25(3):52-8. doi: 10.3109/08820538.2010.488573. Semin Ophthalmol. 2010. PMID: 20590413 Review.
Cited by
-
Modified tarsotomy for the treatment of severe cicatricial entropion.Eye (Lond). 2016 Jul;30(7):992-7. doi: 10.1038/eye.2016.77. Epub 2016 Apr 22. Eye (Lond). 2016. PMID: 27101749 Free PMC article.
-
Outcomes of lower eyelid retractor recession and lateral horn lysis in lower eyelid elevation for facial nerve palsy.Eye (Lond). 2018 Feb;32(2):338-344. doi: 10.1038/eye.2017.174. Epub 2017 Sep 1. Eye (Lond). 2018. PMID: 28862257 Free PMC article.
-
A Comparative Prospective Study of Dermis versus Auricular Cartilage Grafts for the Surgical Correction of Lower Eyelid Retraction.Aesthetic Plast Surg. 2025 Jul 21. doi: 10.1007/s00266-025-04995-6. Online ahead of print. Aesthetic Plast Surg. 2025. PMID: 40691655
-
Bell's phenomenon in thyroid-associated inferior rectus myopathy.Graefes Arch Clin Exp Ophthalmol. 2017 Dec;255(12):2467-2471. doi: 10.1007/s00417-017-3792-9. Epub 2017 Sep 1. Graefes Arch Clin Exp Ophthalmol. 2017. PMID: 28861686
-
A Novel Percutaneous Surgical Approach Using Silicone Sheets for Lower Eyelid Lengthening: A Descriptive Case Series.Plast Reconstr Surg Glob Open. 2025 Mar 17;13(3):e6629. doi: 10.1097/GOX.0000000000006629. eCollection 2025 Mar. Plast Reconstr Surg Glob Open. 2025. PMID: 40110470 Free PMC article.
References
-
- Bartley GB, Kay PP. Posterior lamellar eyelid reconstruction with a hard palate mucosal graft. Am J Ophthalmol. 1989;107:609–12. - PubMed
-
- Baylis HI, Perman KI, Fett DR, et al. Autogenous auricular cartilage grafting for lower eyelid retraction. Ophthal Plast Reconstr Surg. 1985;1:23–7. - PubMed
-
- Ben Simon GJ, Lee S, Schwarcz RM, et al. Subperiosteal midface lift with or without a hard palate mucosal graft for correction of lower eyelid retraction. Ophthalmology. 2006;113:1869–73. - PubMed
-
- Cohen MS, Shorr N. Eyelid reconstruction with hard palate mucosa grafts. Ophthal Plast Reconstr Surg. 1992;8:183–95. - PubMed
-
- Collin JRO, Rathbun JE. Involutional entropion. A review with evaluation of a procesure. Arch Ophthalmol. 1978;96:1058–64. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
