

Effect of operator and institutional volume on clinical outcomes after percutaneous coronary interventions performed in Canada and the United States: a brief report from the Enhanced Suppression of the Platelet glycoprotein IIb/IIIa Receptor with Integrilin Therapy (ESPRIT) study
- PMID: 19668787
- PMCID: PMC2732380
- DOI: 10.1016/s0828-282x(09)70120-5
Effect of operator and institutional volume on clinical outcomes after percutaneous coronary interventions performed in Canada and the United States: a brief report from the Enhanced Suppression of the Platelet glycoprotein IIb/IIIa Receptor with Integrilin Therapy (ESPRIT) study
Abstract
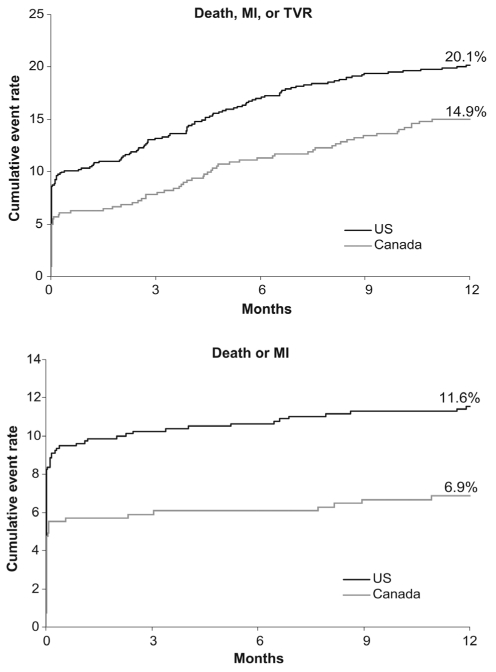
Background: The Enhanced Suppression of the Platelet glycoprotein IIb/IIIa Receptor with Integrilin Therapy (ESPRIT) trial compared the use of eptifibatide with placebo in 2064 coronary intervention patients. It was previously reported that Canadian patients had reduced rates of 30-day and one-year death, myocardial infarction (MI) or target vessel revascularization (TVR) compared with patients in the United States (US).
Objective: To examine whether operator or institutional volume differences explain the regional variation in clinical outcome.
Methods and results: Each site received an operator and institutional volume survey. Fifty-seven sites (62%) returned complete data on 1338 patients. In this smaller cohort, Canadian patients had reduced rates of 30-day and one-year death, MI or TVR compared with US patients (6.3% versus 10.3% and 14.9% versus 20.1%, respectively; P<0.05 for both comparisons). Among 176 physicians with a median of 13 years experience, the median operator volume was 200 cases per year. Operators with fewer than 100 cases per year had higher rates of 30-day death, MI or TVR (13.2% versus 8.7%; P=0.18) and large MI (7.7% versus 3.3%; P=0.06) than those with 100 or more cases per year. The median institutional volume was 1064 cases per year. Canadian and US centres had similar operator and institutional volumes. By multivariate modelling, operator volume was not predictive of adverse clinical events. However, the rates of 30-day and one-year death, MI or TVR fell by 3% for every 100 patients treated by the institution (OR 0.97; P=0.058 and P=0.002, respectively). Enrollment in Canada was associated with improved outcomes at 30 days (OR 0.50; P=0.001) and one year (OR 0.66; P=0.001) despite inclusion of volume variables in the models.
Conclusions: In the ESPRIT study, institutional volume was associated with a modest reduction in risk of death, MI or TVR over short- and long-term follow-up periods. The Canadian and US investigators and institutions selected in ESPRIT had similar annual procedural volumes. Therefore, volume variables did not explain the differential risk of clinical events observed for patients enrolled in the two countries.
HISTORIQUE: L’étude ESPRIT sur la suppression améliorée du récepteur plaquettaire des glycoprotéines IIb/IIIa au moyen d’une thérapie à l’intégriline comparait l’utilisation d’eptifibatide à celle d’un placebo chez 2 064 patients subissant une intervention percutanée. Il avait déjà été établi que les patients du Canada avaient des taux réduits de décès au bout de 30 jours et d’un an, d’infarctus du myocarde (IM) ou de revascularisation de vaisseaux ciblés (RVC) par rapport aux patients des États-Unis.
OBJECTIF: Examiner si les différences entre le volume de l’opérateur ou de l’établissement expliquent la variation régionale en matière d’issues cliniques.
MÉTHODOLOGIE ET RÉSULTATS: Chaque établissement a reçu un sondage sur le volume de l’opérateur et de l’établissement. Cinquante-sept établissements (62 %) ont retourné des données complètes sur 1 338 patients. Dans cette cohorte plus petite, les patients canadiens présentaient un taux réduit de décès au bout de 30 jours et d’un an, d’IM ou de RVC par rapport aux patients des États-Unis (6,3 % par rapport à 10,3 % et 14,9 % par rapport à 20,1 %, respectivement; P<0,05 dans les deux comparaisons). Chez les 176 médecins ayant une expérience médiane de 13 ans, le volume médian de l’opérateur était de 200 cas par année. Les opérateurs voyant moins de 100 cas par année présentaient un taux plus élevé de décès au bout de 30 jours, d’IM ou de RVC (13,2 % par rapport à 8,7 %; P=0,18) et de gros IM (7,7 % par rapport à 3,3 %; P=0,06) que ceux en voyant au moins 100 par année. Le volume médian de l’établissement était de 1 064 cas par année. Les centres canadiens et américains présentaient un volume similaire de l’opérateur et de l’établissement. D’après le modelage multivarié, le volume de l’opérateur n’était pas prédictif des événements cliniques négatifs. Cependant, les taux de décès au bout de 30 jours et d’un an, d’IM et de RVC diminuaient de 3 % par tranche de 100 patients traités par l’établissement (RRR 0,97; P=0,058 et P=0,002, respectivement). La participation au Canada s’associait à une meilleure issue au bout de 30 jours (RRR 0,50; P=0,001) et d’un an (RRR 0,66; P=0,01) malgré l’inclusion des variables de volume dans le modèle.
CONCLUSIONS: Dans l’étude ESPRIT, le volume de l’établissement s’associait à une modeste réduction du risque de décès, d’IM ou de RVC pendant des périodes de suivi à court et à long terme. Les médecins et les établissements canadiens et américains sélectionnés pour l’étude ESPRIT présentaient un volume annuel similaire d’interventions. Ainsi, les variables de volume n’expliquaient pas le risque différentiel d’événements cliniques observé chez les patients des deux pays.
Figures
References
-
- Kimmel SE, Berlin JA, Laskey WK. The relationship between coronary angioplasty procedure volume and major complications. JAMA. 1995;274:1137–42. - PubMed
-
- Jollis JG, Peterson ED, DeLong ER, et al. The relationship between the volume of coronary angioplasty procedures at hospitals treating Medicare beneficiaries and short term mortality. N Engl J Med. 1994;331:1625–9. - PubMed
-
- Hannan EL, Racz M, Ryan TJ, et al. Coronary angioplasty volume-outcome relationships for hospitals and cardiologists. JAMA. 1997;277:892–8. - PubMed
-
- Hannan EL, Wu C, Walford G, et al. Volume-outcome relationships for percutaneous coronary interventions in the stent era. Circulation. 2005;112:1171–9. - PubMed
-
- McGrath PD, Wennberg DE, Malenka DJ, et al. for the Northern New England Cardiovascular Disease Study Group. Operator volume and outcomes in 12,988 percutaneous coronary interventions. J Am Coll Cardiol. 1998;31:570–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
