

Anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis in children and adolescents
- PMID: 19670433
- PMCID: PMC2826225
- DOI: 10.1002/ana.21756
Anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis in children and adolescents
Abstract
Objective: To report the clinical features of anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis in patients < or = 18 years old.
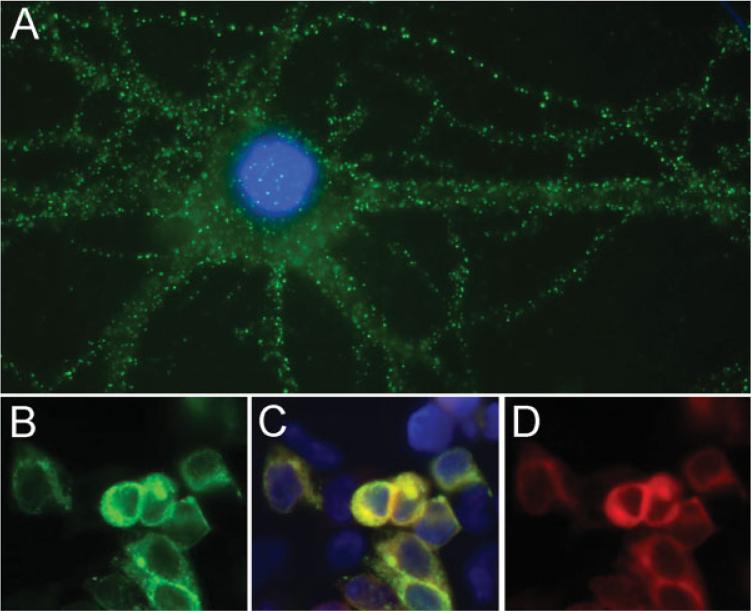
Methods: Information was obtained by the authors or referring physicians. Antibodies were determined by immunocytochemistry and enzyme-linked immunosorbent assay (ELISA) using HEK293 cells ectopically expressing NR1.
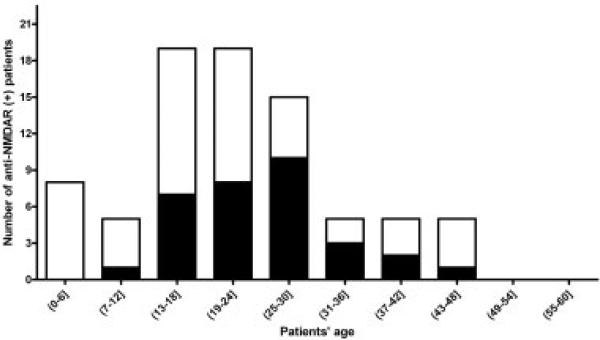
Results: Over an 8-month period, 81 patients (12 male) with anti-NMDAR encephalitis were identified. Thirty-two (40%) were < or =18 years old (youngest 23 months, median 14 years); 6 were male. The frequency of ovarian teratomas was 56% in women >18 years old, 31% in girls < or =18 years old (p = 0.05), and 9% in girls < or =14 years old (p = 0.008). None of the male patients had tumors. Of 32 patients < or =18 years old, 87.5% presented with behavioral or personality change, sometimes associated with seizures and frequent sleep dysfunction; 9.5% with dyskinesias or dystonia; and 3% with speech reduction. On admission, 53% had severe speech deficits. Eventually, 77% developed seizures, 84% stereotyped movements, 86% autonomic instability, and 23% hypoventilation. Responses to immunotherapy were slow and variable. Overall, 74% had full or substantial recovery after immunotherapy or tumor removal. Neurological relapses occurred in 25%. At the last follow-up, full recovery occurred more frequently in patients who had a teratoma that was removed (5/8) than in those without a teratoma (4/23; p = 0.03).
Interpretation: Anti-NMDAR encephalitis is increasingly recognized in children, comprising 40% of all cases. Younger patients are less likely to have tumors. Behavioral and speech problems, seizures, and abnormal movements are common early symptoms. The phenotype resembles that of the adults, although dysautonomia and hypoventilation are less frequent or severe in children. Ann Neurol 2009;66:11-18.
Figures


Comment in
-
In search of lost time from "Demonic Possession" to anti-N-methyl-D-aspartate receptor encephalitis.Ann Neurol. 2010 Jan;67(1):141-2; author reply 142-3. doi: 10.1002/ana.21928. Ann Neurol. 2010. PMID: 20186949 No abstract available.
References
-
- Tonomura Y, Kataoka H, Hara Y, et al. Clinical analysis of paraneoplastic encephalitis associated with ovarian teratoma. J Neurooncol. 2007;84:287–292. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
