

Transpulmonary thermodilution-derived cardiac function index identifies cardiac dysfunction in acute heart failure and septic patients: an observational study
- PMID: 19671146
- PMCID: PMC2750191
- DOI: 10.1186/cc7994
Transpulmonary thermodilution-derived cardiac function index identifies cardiac dysfunction in acute heart failure and septic patients: an observational study
Abstract
Introduction: There is limited clinical experience with the single-indicator transpulmonary thermodilution (pulse contour cardiac output, or PiCCO) technique in critically ill medical patients, particularly in those with acute heart failure (AHF). Therefore, we compared the cardiac function of patients with AHF or sepsis using the pulmonary artery catheter (PAC) and the PiCCO technology.
Methods: This retrospective observational study was conducted in the medical intensive care unit of a university hospital. Twelve patients with AHF and nine patients with severe sepsis or septic shock had four simultaneous hemodynamic measurements by PAC and PiCCO during a 24-hour observation period. Comparisons between groups were made with the use of the Mann-Whitney U test. Including all measurements, correlations between data pairs were established using linear regression analysis and are expressed as the square of Pearson's correlation coefficients (r2).
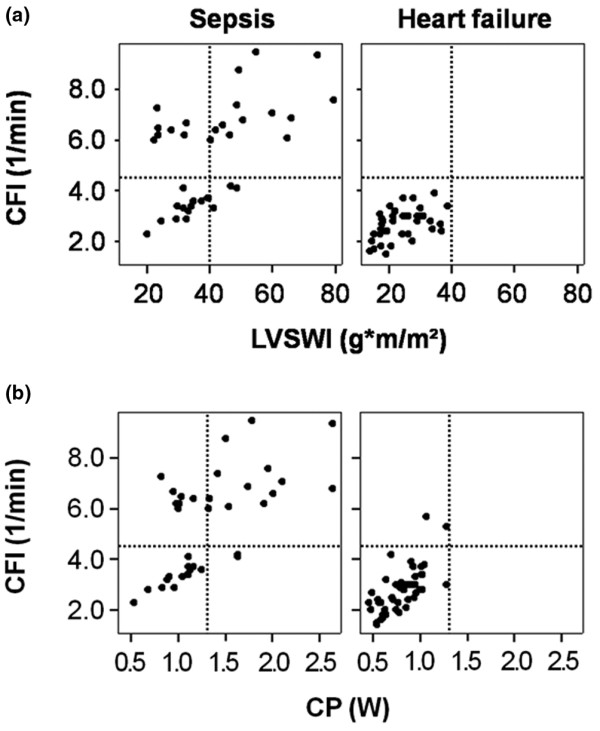
Results: Compared to septic patients, AHF patients had a significantly lower cardiac index, cardiac function index (CFI), global ejection fraction, mixed venous oxygen saturation (SmvO2) and pulmonary vascular permeability index, but higher pulmonary artery occlusion pressure. All patients with a CFI less than 4.5 per minute had an SmvO2 not greater than 70%. In both groups, the CFI correlated with the left ventricular stroke work index (sepsis: r2 = 0.30, P < 0.05; AHF: r2 = 0.23, P < 0.05) and cardiac power (sepsis: r2 = 0.39, P < 0.05; AHF: r2 = 0.45, P < 0.05).
Conclusions: In critically ill medical patients, assessment of cardiac function using transpulmonary thermodilution technique is an alternative to the PAC. A low CFI identifies cardiac dysfunction in both AHF and septic patients.
Figures



Comment in
-
Pulmonary artery catheters in acute heart failure: end of an era?Crit Care. 2009;13(6):1003. doi: 10.1186/cc8113. Epub 2009 Nov 11. Crit Care. 2009. PMID: 19930618 Free PMC article.
References
-
- Binanay C, Califf RM, Hasselblad V, O'Connor CM, Shah MR, Sopko G, Stevenson LW, Francis GS, Leier CV, Miller LW. Evaluation study of congestive heart failure and pulmonary artery catheterization effectiveness: the ESCAPE trial. JAMA. 2005;294:1625–1633. doi: 10.1001/jama.294.13.1625. - DOI - PubMed
-
- Richard C, Warszawski J, Anguel N, Deye N, Combes A, Barnoud D, Boulain T, Lefort Y, Fartoukh M, Baud F, Boyer A, Brochard L, Teboul JL. Early use of the pulmonary artery catheter and outcomes in patients with shock and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2003;290:2713–2720. doi: 10.1001/jama.290.20.2713. - DOI - PubMed
-
- Harvey S, Harrison DA, Singer M, Ashcroft J, Jones CM, Elbourne D, Brampton W, Williams D, Young D, Rowan K. Assessment of the clinical effectiveness of pulmonary artery catheters in management of patients in intensive care (PAC-Man): a randomised controlled trial. Lancet. 2005;366:472–477. doi: 10.1016/S0140-6736(05)67061-4. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
