

Does postoperative delirium limit the use of patient-controlled analgesia in older surgical patients?
- PMID: 19672166
- PMCID: PMC2762324
- DOI: 10.1097/ALN.0b013e3181acf7e6
Does postoperative delirium limit the use of patient-controlled analgesia in older surgical patients?
Abstract
BACKGROUNDPostoperative pain Is an independent predictor of postoperative delirium. Whether postoperative delirium limits patient-controlled analgesia (PCA) use has not been determined.
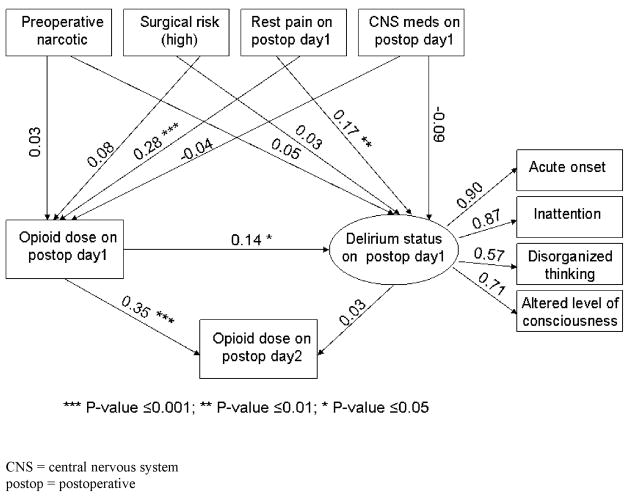
Methods: The authors conducted a nested cohort study in older patients undergoing noncardiac surgery and used PCA for postoperative analgesia. Delirium was measured by using the Confusion Assessment Method. The authors computed a structural equation model to determine the effects of pain and opioid consumption on delirium status and the effect of delirium on opioid use.
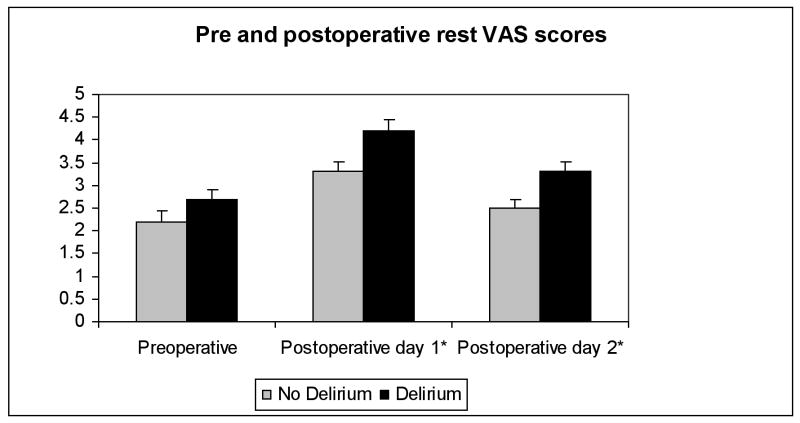
Results: Of 335 patients, 108 (32.2%) developed delirium on postoperative day (POD) 1, and 120 (35.8%) on POD 2. Postoperative delirium did not limit the use of PCA. Patients with postoperative delirium used more PCA in a 24-h period (POD 2) compared to those without delirium (mean dose of hydromorphone +/- SE adjusted for covariates was 2.24 +/- 0.71 mg vs. 1.25 +/- 0.67 mg, P = 0.02). Despite more opioid use, patients with delirium reported higher Visual Analogue Scale scores than those without delirium (POD 1: mean visual analog scale +/- SE at rest 4.2 +/- 0.23 vs. 3.3 +/- 0.22, P = 0.0051; POD 2: 3.3 +/- 0.23 vs. 2.5 +/- 0.19, P = 0.004). Path coefficients from structural equation model revealed that pain and opioid use affect delirium status, but delirium does not affect subsequent opioid dose.
Conclusions: Postoperative delirium did not limit PCA use. Despite more opioid use, visual analog scale scores were higher in patients with delirium. Future studies on delirium should consider the role of pain and pain management as potential etiologic factors.
Figures
References
-
- Lipowski Z. Delirium (acute confusional states) JAMA. 1987;258:1789–92. - PubMed
-
- Lipowski Z. Delirium in the elderly patient. New Engl J Med. 1989;320:578–82. - PubMed
-
- Inouye S. The dilemma of delirium: clinical and research controversies regarding diagnosis and evaluation of delirium in hospitalized elderly medical patients. Am J Med. 1994;97:278–88. - PubMed
-
- Parikh S, Chung C. Postoperative delirium in the elderly. Anesth Analg. 1995;80:1223–32. - PubMed
-
- Brauer C, Morrison RS, Silberzweig SB, Siu AL. The cause of delirium in patients with hip fracture. Arch Intern Med. 2000;160:1856–60. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
