

A multifaceted strategy for implementation of the Ottawa ankle rules in two emergency departments
- PMID: 19675080
- PMCID: PMC2726279
- DOI: 10.1136/bmj.b3056
A multifaceted strategy for implementation of the Ottawa ankle rules in two emergency departments
Abstract
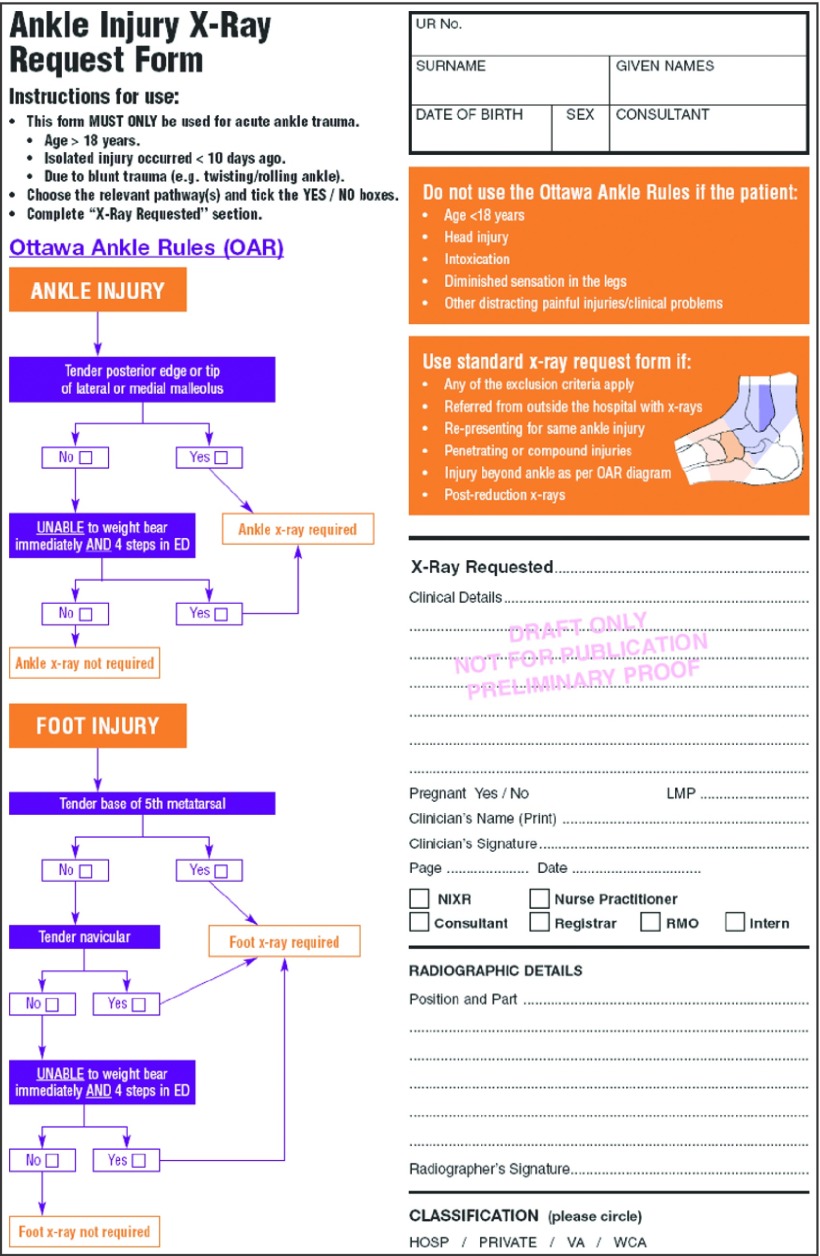
Problem: Despite widespread acceptance of the Ottawa ankle rules for assessment of acute ankle injuries, their application varies considerably.
Design: Before and after study.
Background and setting: Emergency departments of a tertiary teaching hospital and a community hospital in Australia.
Key measures for improvement: Documentation of the Ottawa ankle rules, proportion of patients referred for radiography, proportion of radiographs showing a fracture.
Strategies for change: Education, a problem specific radiography request form, reminders, audit and feedback, and using radiographers as "gatekeepers."
Effects of change: Documentation of the Ottawa ankle rules improved from 57.5% to 94.7% at the tertiary hospital, and 51.6% to 80.8% at the community hospital (P<0.001 for both). The proportion of patients undergoing radiography fell from 95.8% to 87.2% at the tertiary hospital, and from 91.4% to 78.9% at the community hospital (P<0.001 for both). The proportion of radiographs showing a fracture increased from 20.4% to 27.1% at the tertiary hospital (P=0.069), and 15.2% to 27.2% (P=0.002) at the community hospital. The missed fracture rate increased from 0% to 2.9% at the tertiary hospital and from 0% to 1.6% at the community hospital compared with baseline (P=0.783 and P=0.747).
Lessons learnt: Assessment of case note documentation has limitations. Clinician groups seem to differ in their capacity and willingness to change their practice. A multifaceted change strategy including a problem specific radiography request form can improve the selection of patients for radiography.
Conflict of interest statement
Competing interests: None declared.
Comment in
-
Evidence based implementation of complex interventions.BMJ. 2009 Aug 12;339:b3124. doi: 10.1136/bmj.b3124. BMJ. 2009. PMID: 19675081 No abstract available.
References
-
- Dopson S, FitzGerald L, Ferlie E, Gabbay J, Locock L. No magic targets! Changing clinical practice to become more evidence based. Health Care Manage Rev 2002;27:35-47. - PubMed
-
- Sanson-Fisher RW. Diffusion of innovation theory for clinical change. Med J Aust 2004;180(suppl):S55-6. - PubMed
-
- Stiell IG, McKnight RD, Greenberg GH, McDowell I, Nair RC, Wells GA, et al. Implementation of the Ottawa ankle rules. JAMA 1994;271:827-32. - PubMed
-
- Stiell IG, Greenberg GH, McKnight RD, Nair RC, McDowell I, Reardon M, et al. Decision rules for the use of radiography in acute ankle injuries: refinement and prospective validation. JAMA 1993;269:1127-32. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials