

Increased cerebral blood volume and oxygen consumption in neonatal brain injury
- PMID: 19675563
- PMCID: PMC2762197
- DOI: 10.1038/jcbfm.2009.90
Increased cerebral blood volume and oxygen consumption in neonatal brain injury
Abstract
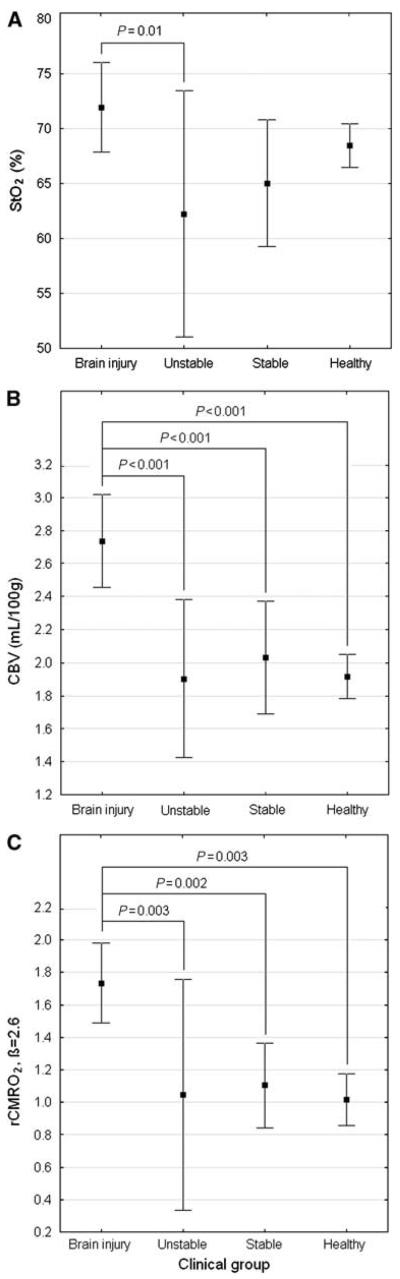
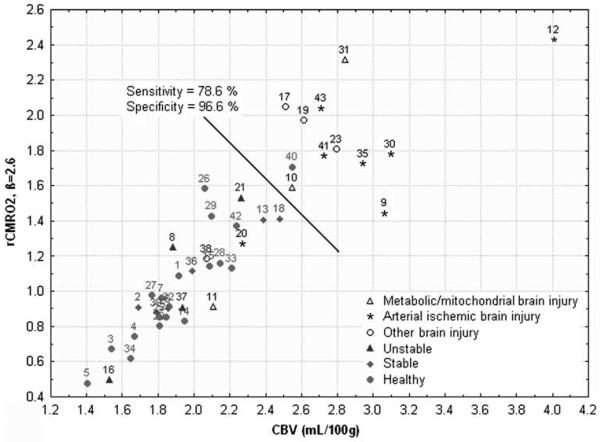
With the increasing interest in treatments for neonatal brain injury, bedside methods for detecting and assessing injury status and evolution are needed. We aimed to determine whether cerebral tissue oxygenation (StO(2)), cerebral blood volume (CBV), and estimates of relative cerebral oxygen consumption (rCMRO(2)) determined by bedside frequency-domain near-infrared spectroscopy (FD-NIRS) have the potential to distinguish neonates with brain injury from those with non-brain issues and healthy controls. We recruited 43 neonates < or =15 days old and >33 weeks gestational age (GA): 14 with imaging evidence of brain injury, 29 without suspicion of brain injury (4 unstable, 6 stable, and 19 healthy). A multivariate analysis of variance with Newman-Keuls post hoc comparisons confirmed group similarity for GA and age at measurement. StO(2) was significantly higher in brain injured compared with unstable neonates, but not statistically different from stable or healthy neonates. Brain-injured neonates were distinguished from all others by significant increases in CBV and rCMRO(2). In conclusion, although NIRS measures of StO(2) alone may be insensitive to evolving brain injury, increased CBV and rCMRO(2) seem to be useful for detecting neonatal brain injury and suggest increased neuronal activity and metabolism occurs acutely in evolving brain injury.
Figures
Similar articles
-
Noninvasive optical measures of CBV, StO(2), CBF index, and rCMRO(2) in human premature neonates' brains in the first six weeks of life.Hum Brain Mapp. 2010 Mar;31(3):341-52. doi: 10.1002/hbm.20868. Hum Brain Mapp. 2010. PMID: 19650140 Free PMC article.
-
Near-infrared spectroscopy assessment of cerebral oxygen metabolism in the developing premature brain.J Cereb Blood Flow Metab. 2012 Mar;32(3):481-8. doi: 10.1038/jcbfm.2011.145. Epub 2011 Oct 26. J Cereb Blood Flow Metab. 2012. PMID: 22027937 Free PMC article.
-
Simultaneous measurement of cerebral hemoglobin oxygen saturation and blood volume in asphyxiated neonates by near-infrared time-resolved spectroscopy.Brain Dev. 2015 Nov;37(10):925-32. doi: 10.1016/j.braindev.2015.04.002. Epub 2015 May 11. Brain Dev. 2015. PMID: 25975705
-
Evaluation of cerebral circulation and oxygen metabolism in infants using near-infrared light.Brain Dev. 2014 Apr;36(4):277-83. doi: 10.1016/j.braindev.2013.05.011. Epub 2013 Jun 22. Brain Dev. 2014. PMID: 23800410 Review.
-
Near infrared spectroscopy in brain injury: today's perspective.Acta Neurochir Suppl. 2005;95:453-7. doi: 10.1007/3-211-32318-x_93. Acta Neurochir Suppl. 2005. PMID: 16463900 Review.
Cited by
-
Near-infrared spectroscopy versus magnetic resonance imaging to study brain perfusion in newborns with hypoxic-ischemic encephalopathy treated with hypothermia.Neuroimage. 2014 Jan 15;85 Pt 1(0 1):287-93. doi: 10.1016/j.neuroimage.2013.04.072. Epub 2013 Apr 28. Neuroimage. 2014. PMID: 23631990 Free PMC article.
-
Optical imaging in vivo with a focus on paediatric disease: technical progress, current preclinical and clinical applications and future perspectives.Pediatr Radiol. 2011 Feb;41(2):161-75. doi: 10.1007/s00247-010-1907-0. Epub 2011 Jan 11. Pediatr Radiol. 2011. PMID: 21221568 Free PMC article. Review.
-
Noninvasive optical measures of CBV, StO(2), CBF index, and rCMRO(2) in human premature neonates' brains in the first six weeks of life.Hum Brain Mapp. 2010 Mar;31(3):341-52. doi: 10.1002/hbm.20868. Hum Brain Mapp. 2010. PMID: 19650140 Free PMC article.
-
Imaging of an inflammatory injury in the newborn rat brain with photoacoustic tomography.PLoS One. 2013 Dec 26;8(12):e83045. doi: 10.1371/journal.pone.0083045. eCollection 2013. PLoS One. 2013. PMID: 24386140 Free PMC article.
-
Esophageal reflexes modulate frontoparietal response in neonates: Novel application of concurrent NIRS and provocative esophageal manometry.Am J Physiol Gastrointest Liver Physiol. 2014 Jul 1;307(1):G41-9. doi: 10.1152/ajpgi.00350.2013. Epub 2014 May 1. Am J Physiol Gastrointest Liver Physiol. 2014. PMID: 24789204 Free PMC article.
References
-
- al Naqeeb N, Edwards AD, Cowan FM, Azzopardi D. Assessment of neonatal encephalopathy by amplitude-integrated electroencephalography. Pediatrics. 1999;103:1263–71. - PubMed
-
- Altman DI, Volpe JJ. Positron emission tomography in newborn infants. Clin Perinatol. 1991;18:549–62. - PubMed
-
- Austin T, Gibson AP, Branco G, Yusof RM, Arridge SR, Meek JH, Wyatt JS, Delpy DT, Hebden JC. Three dimensional optical imaging of blood volume and oxygenation in the neonatal brain. Neuroimage. 2006;31:1426–33. - PubMed
-
- Benaron DA, Benitz WE, Ariagno RA, Stevenson DK. Noninvasive methods for estimating in vivo oxigenation. Clin Pediatr. 1992;31:258–73. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
