

The impact of IPTi and IPTc interventions on malaria clinical burden - in silico perspectives
- PMID: 19675675
- PMCID: PMC2722080
- DOI: 10.1371/journal.pone.0006627
The impact of IPTi and IPTc interventions on malaria clinical burden - in silico perspectives
Abstract
Background: Clinical management of malaria is a major health issue in sub-Saharan Africa. New strategies based on intermittent preventive treatment (IPT) can tackle disease burden by simultaneously reducing frequency of infections and life-threatening illness in infants (IPTi) and children (IPTc), while allowing for immunity to build up. However, concerns as to whether immunity develops efficiently in treated individuals, and whether there is a rebound effect after treatment is halted, have made it imperative to define the effects that IPTi and IPTc exert on the clinical malaria scenario.
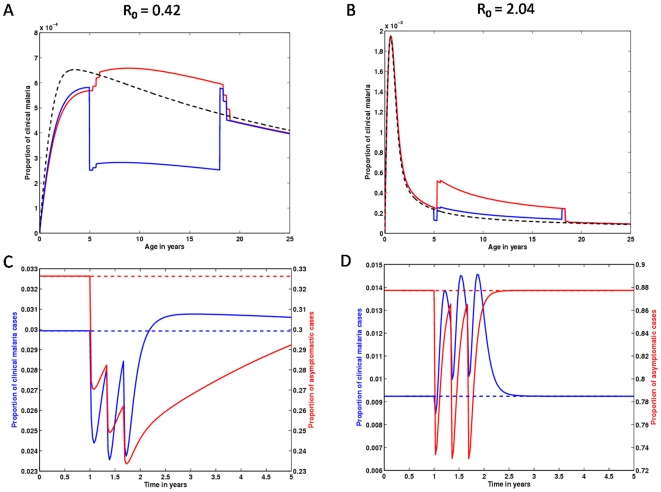
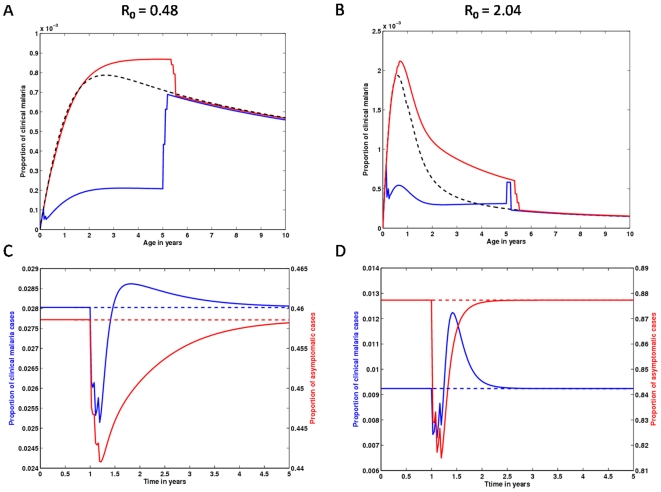
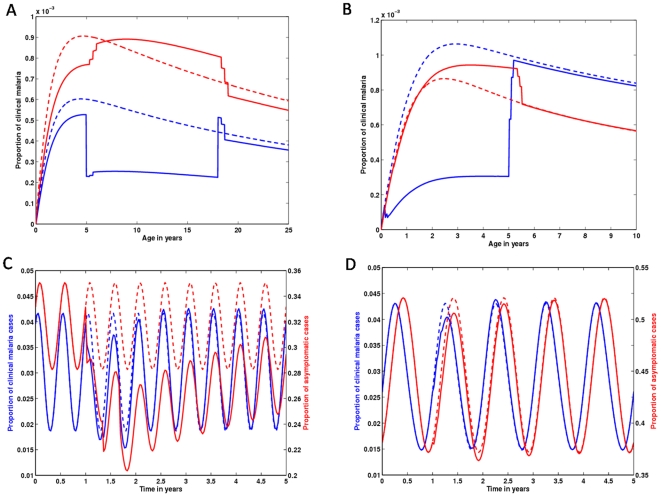
Methods and findings: Here, we simulate several schemes of intervention under different transmission settings, while varying immunity build up assumptions. Our model predicts that infection risk and effectiveness of acquisition of clinical immunity under prophylactic effect are associated to intervention impact during treatment and follow-up periods. These effects vary across regions of different endemicity and are highly correlated with the interplay between the timing of interventions in age and the age dependent risk of acquiring an infection. However, even when significant rebound effects are predicted to occur, the overall intervention impact is positive.
Conclusions: IPTi is predicted to have minimal impact on the acquisition of clinical immunity, since it does not interfere with the occurrence of mild infections, thus failing to reduce the underlying force of infection. On the contrary, IPTc has a significant potential to reduce transmission, specifically in areas where it is already low to moderate.
Conflict of interest statement
Figures
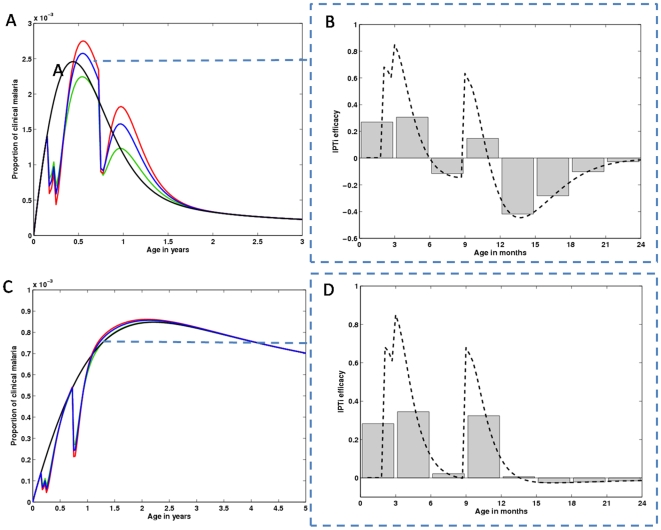
 (green line) to
(green line) to  (red line). The blue line represents the intermediate combination,
(red line). The blue line represents the intermediate combination,  . (B) The dashed line represents the age instantaneous intervention efficacy for the blue curve scenario in (A). The grey bars illustrate efficacy over a 3 months range. (C) Represents the same as in (A), but for a intermediate transmission setting. (D) The dashed line represents the age instantaneous intervention efficacy for the blue curve scenario in (C). The grey bars illustrate efficacy over a 3 months period.
. (B) The dashed line represents the age instantaneous intervention efficacy for the blue curve scenario in (A). The grey bars illustrate efficacy over a 3 months range. (C) Represents the same as in (A), but for a intermediate transmission setting. (D) The dashed line represents the age instantaneous intervention efficacy for the blue curve scenario in (C). The grey bars illustrate efficacy over a 3 months period.
Similar articles
-
Determinants of the cost-effectiveness of intermittent preventive treatment for malaria in infants and children.PLoS One. 2011 Apr 7;6(4):e18391. doi: 10.1371/journal.pone.0018391. PLoS One. 2011. PMID: 21490967 Free PMC article.
-
Intermittent preventive treatment for malaria in infants: a decision-support tool for sub-Saharan Africa.Bull World Health Organ. 2010 Nov 1;88(11):807-14. doi: 10.2471/BLT.09.072397. Epub 2010 May 10. Bull World Health Organ. 2010. PMID: 21076561 Free PMC article.
-
Modelling the epidemiological impact of intermittent preventive treatment against malaria in infants.PLoS One. 2008 Jul 16;3(7):e2661. doi: 10.1371/journal.pone.0002661. PLoS One. 2008. PMID: 18628828 Free PMC article.
-
Intermittent preventive treatment of malaria in infants: how does it work and where will it work?Trop Med Int Health. 2009 Sep;14(9):1003-10. doi: 10.1111/j.1365-3156.2009.02303.x. Epub 2009 Jun 22. Trop Med Int Health. 2009. PMID: 19558374 Review.
-
The promise and potential challenges of intermittent preventive treatment for malaria in infants (IPTi).Malar J. 2005 Jul 20;4:33. doi: 10.1186/1475-2875-4-33. Malar J. 2005. PMID: 16033653 Free PMC article. Review.
Cited by
-
Intermittent Preventive Treatment (IPT): Its Role in Averting Disease-Induced Mortality in Children and in Promoting the Spread of Antimalarial Drug Resistance.Bull Math Biol. 2019 Jan;81(1):193-234. doi: 10.1007/s11538-018-0524-1. Epub 2018 Oct 31. Bull Math Biol. 2019. PMID: 30382460 Free PMC article.
-
Anti-malarial market and policy surveys in sub-Saharan Africa.Malar J. 2010 Apr 23;9 Suppl 1(Suppl 3):S1. doi: 10.1186/1475-2875-9-S1-S1. Malar J. 2010. PMID: 20423536 Free PMC article.
-
Modeling malaria infection and immunity against variant surface antigens in Príncipe Island, West Africa.PLoS One. 2014 Feb 10;9(2):e88110. doi: 10.1371/journal.pone.0088110. eCollection 2014. PLoS One. 2014. PMID: 24520349 Free PMC article.
-
Anti-malarial drugs and the prevention of malaria in the population of malaria endemic areas.Malar J. 2010 Dec 13;9 Suppl 3(Suppl 3):S2. doi: 10.1186/1475-2875-9-S3-S2. Malar J. 2010. PMID: 21144082 Free PMC article. Review.
-
Public health impact of current and proposed age-expanded perennial malaria chemoprevention: a modelling study.Sci Rep. 2025 Mar 26;15(1):10488. doi: 10.1038/s41598-025-93623-z. Sci Rep. 2025. PMID: 40140443 Free PMC article.
References
-
- Greenwood B. The use of anti-malarial drugs to prevent malaria in the population of malaria-endemic regions. Am J Trop Med Hyg. 2004;70(1):1–7. - PubMed
-
- Myint HY, Tipmanee P, Nosten F, Day NP, Pukrittayakamee S, et al. A systematic overview of published antimalarial drug trials. Trans R Soc Trop Med Hyg. 2004;98(2):73–81. - PubMed
-
- Menendez C, Kahigwa E, Hirt R, Vounatsou P, Aponte JJ, et al. Randomised placebo-controlled trial of iron supplementation and malaria chemoprophylaxis for prevention of severe anaemia and malaria in Tanzanian infants. Lancet. 1997;350(9081):844–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
