

Preclinical care of children with traumatic brain injury (TBI)
- PMID: 19675685
- PMCID: PMC2703212
Preclinical care of children with traumatic brain injury (TBI)
Abstract
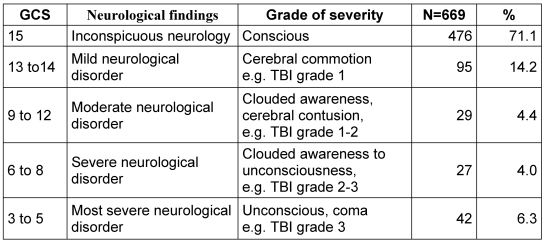
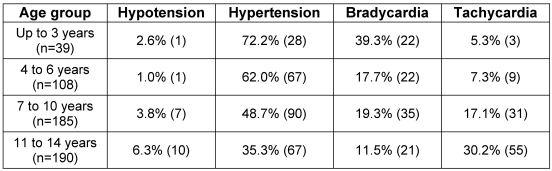
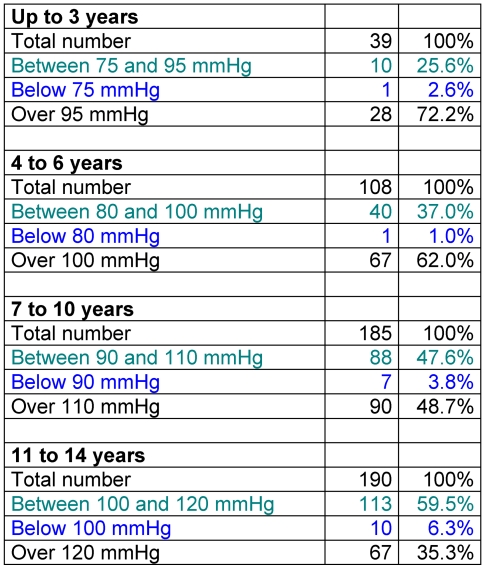
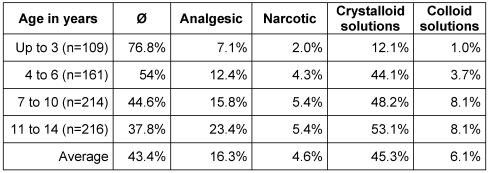
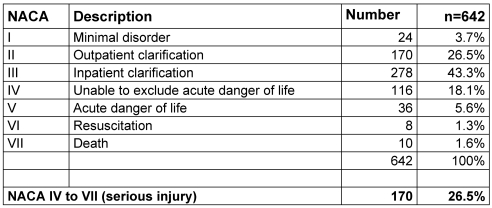
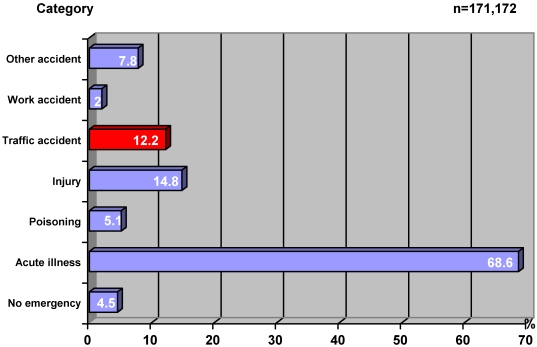
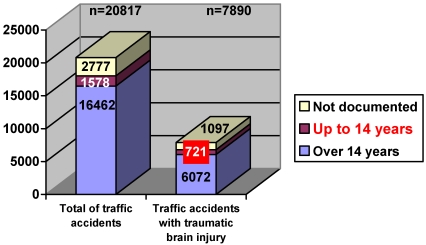
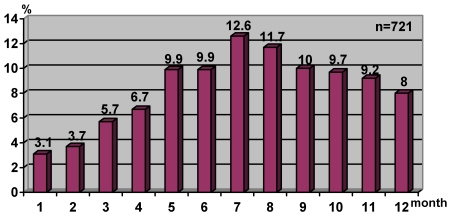
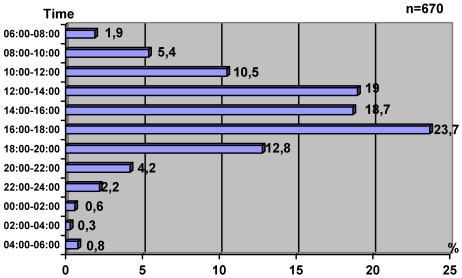
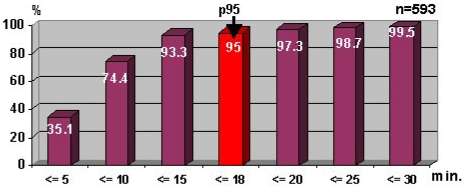
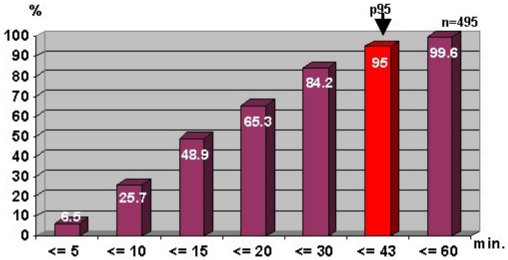
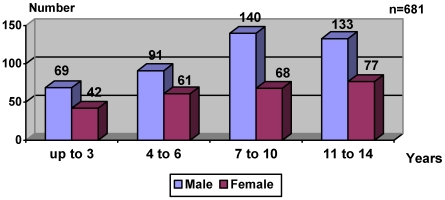
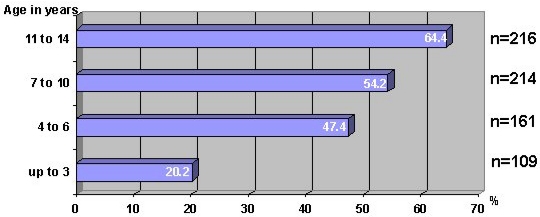
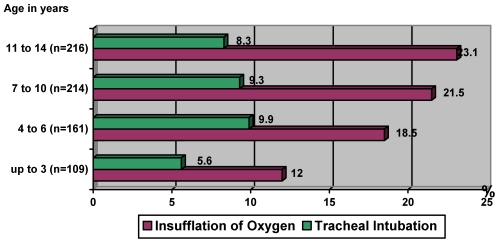
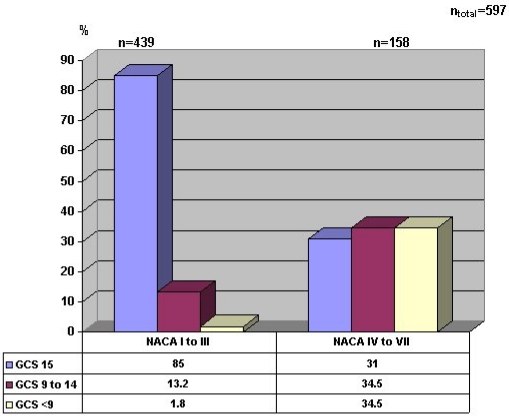
The fact that injuries caused by accidents are the most common cause of death in children and adolescents in Germany gave rise to the study, which mainly deals with traffic accidents in this group. 200,221 records of emergency-service physicians in Bavaria which cover the period 1995-1999 were analysed with respect to the importance of traumatic brain injury (TBI) in children and adolescents (n = 721 - representing 45.8% of traffic injuries in this age group). The highest incidence of TBI was in summer (34.3%) and in the evening between 16.00 and 18.00 (23.7%). The time taken between accident and arrival of the emergency services was 8.8 +/- 3.1 minutes. The preclinical phase lasted 19.3 +/- 5.8 minutes. The probability of having an accident with TBI increases with age, the maximum being in the age-range 7 - 14 years (61.6%). Boys (63.2%) were almost twice as susceptible to injury as girls. 36.8% of all cases had no noticeable neurological disorder, 71.1% resulted in a Glasgow Coma Scale (GCS) score of 15. Only 6.3% had most severe neurological disorders, resulting in a GCS score of 3 - 5. Circulation parameters in the form of adapted hypotension were abnormal in only 3.4%, 21.9% of the children had a bradycardia and in 12.3% the blood oxygen saturation fell below 94%. The most frequent intervention was the laying of an i.v. line for infusions. 8.6% of the patients were intubated to allow for ventilation with oxygen. Analgesics were given in 16.7% of the cases. In 84.7% of all cases, the condition was stable and in only 3.3% was a severe deterioration to be observed. The assessments were made using both the National Advisory Committee for Aeronautics (NACA) and Glasgow Coma Scales (GCS). Discrepancies occurred, as a NACA scale of I - III and a GCS score of < 9 was reported in 4.9% of cases. In contrast a NACA scale of IV - VI was reported with a GCS score of 15 in 30% of all cases. TBI symptoms in children are less obvious than in adults, which leads to an age-dependent restriction in implementing therapeutic measures. If these restrictions are a result of misinterpretation of the situation or due to a lack of practice in the preclinical phase, then further training and education of the physicians involved in emergency service work are necessary.
Vor dem Hindergrund der Tatsache, dass unfallbedingte Verletzungen die häufigste Todesursache im Kindes- und Jugendalter in Deutschland sind, wurde das Patientenkollektiv des Notarztdienstes in Bayern (n = 200.221) analysiert mit der Frage des Stellenwertes des Schädelhirntraumas (SHT). In den Notarztprotokollen fanden sich 721 Kinder mit SHT, das waren 45,8% der kindlichen Verkehrsunfälle. Der Häufigkeitsgipfel war in den Sommermonaten (34,3%), während die täglichen Einsatzspitzen am Nachmittag zwischen 16:00 und 18:00 Uhr (23,7%) lagen. Die durchschnittliche Eintreffzeit des Notarztes liegt in Bayern bei 8,8 Minuten (± 3,1 Min.), während für die präklinische Therapie am Notfallort (vor Abfahrt des Rettungswagens) durchschnittlich 19,3 Minuten (± 5,8 Min) benötigt wurden. Mit zunehmendem Alter steigt der Anteil der verunglückten Kinder mit einer deutlichen Betonung der 7 - 14-Jährigen (61,6%). Jungen sind doppelt so häufig verunfallt (63,6%) wie Mädchen. 36,8% der Kinder waren neurologisch unauffällig, während für 71,1% ein GCS-Wert von 15 dokumentiert wurde. Nur 6,3% hatten schwerste neurologische Störungen (GCS 3 - 5). Die Kreislaufparameter wichen nur in 3,4% von der Norm im Sinne einer kindlich adaptierten Hypotonie ab. Auch eine Bradykardie betraf nur 21,9% der Kinder. Lediglich 12,3% wiesen einen Abfall der Sauerstoffsättigung des Blutes auf unter 94% auf. Die häufigste Maßnahme war das Anlegen einer Infusion, die jedes zweite Kind (49,6%) erhielt. Allerdings war bei dieser Maßnahme eine deutliche Altersabhängigkeit auszumachen, was auch für die Applikation von Sauerstoff als Therapiemaßnahme zutrifft. Unabhängig vom Alter wurde fast jedes zehnte Kind intubiert (8,6%). Eine altersabhängige Zurückhaltung war auch bei der medikamentösen Analgesierung auszumachen, die insgesamt nur in 16,7% der Fälle erfolgte. Insgesamt konnte der Zustand der Kinder bis zur Klinikübergabe in 84,7% der Fälle gehalten werden, nur in 3,3% kam es zu einer Verschlechterung. Bei einem Vergleich zwischen der subjektiven Beurteilung des Notarztes mittels der NACA-Skala und dem GCS-Wert werden deutliche Diskrepanzen offenbar, wenn bei einem NACA von I - III in 4,9% ein GCS-Wert von unter 9 und umgekehrt bei einem NACA von IV - VI ein GCS-Wert von 15 bei 30% vorlag. Im Gegensatz zu Erwachsenen sind die Leitsymptome des SHT bei Kindern nicht so deutlich, was zu einer altersabhängigen Zurückhaltung bei den therapeutischen Maßnahmen führt. Ob diese Zurückhaltung ausschließlich auf einer Fehleinschätzung der Dringlichkeit oder aber auf mangelnder Praxis bei der präklinischen Durchführung der Therapie beruht, bleibt offen, macht aber eine dringende Fortbildungsnotwendigkeit deutlich.
Figures
References
-
- Helm M, Haucke J, Frey W, Lampl L. Der pädiatrische Traumapatient im Luftrettungsdienst: alterspezifische Besonderheiten. Notfall Rettungsmed. 1999;2(3):150–157.
-
- Maier-Hauff K, Gatzounis G, Borschel M. Das kindliche Schädel-Hirn-Trauma. Besonderheiten, Therapie und Prognose. Unfallchirurg. 1993;96(11):604–608. - PubMed
-
- Schulte FJ, Spranger J. Unfälle im Kindesalter. In: Schulte FJ, editor. Lehrbuch der Kinderheilkunde. 27. Aufl. Stuttgart: Fischer; 1993. pp. 905–912.
-
- Scheingraber S, Reulen HJ. Praxis präklinischer Versorgung Schädel-Hirn-Traumatisierter. Notfall Rettungsmed. 1999;2(2):84–91.
-
- Hall SC. Pediatric trauma in the 90s: an overview. Int Anesthesiol Clin. 1994;32(1):1–9. - PubMed
LinkOut - more resources
Full Text Sources