

Photodynamic therapy (PDT) and waterfiltered infrared A (wIRA) in patients with recalcitrant common hand and foot warts
- PMID: 19675691
- PMCID: PMC2703213
Photodynamic therapy (PDT) and waterfiltered infrared A (wIRA) in patients with recalcitrant common hand and foot warts
Abstract
Background: Common warts (verrucae vulgares) are human papilloma virus (HPV) infections with a high incidence and prevalence, most often affecting hands and feet, being able to impair quality of life. About 30 different therapeutic regimens described in literature reveal a lack of a single striking strategy. Recent publications showed positive results of photodynamic therapy (PDT) with 5-aminolevulinic acid (5-ALA) in the treatment of HPV-induced skin diseases, especially warts, using visible light (VIS) to stimulate an absorption band of endogenously formed protoporphyrin IX. Additional experiences adding waterfiltered infrared A (wIRA) during 5-ALA-PDT revealed positive effects.
Aim of the study: First prospective randomised controlled blind study including PDT and wIRA in the treatment of recalcitrant common hand and foot warts. Comparison of "5-ALA cream (ALA) vs. placebo cream (PLC)" and "irradiation with visible light and wIRA (VIS+wIRA) vs. irradiation with visible light alone (VIS)".
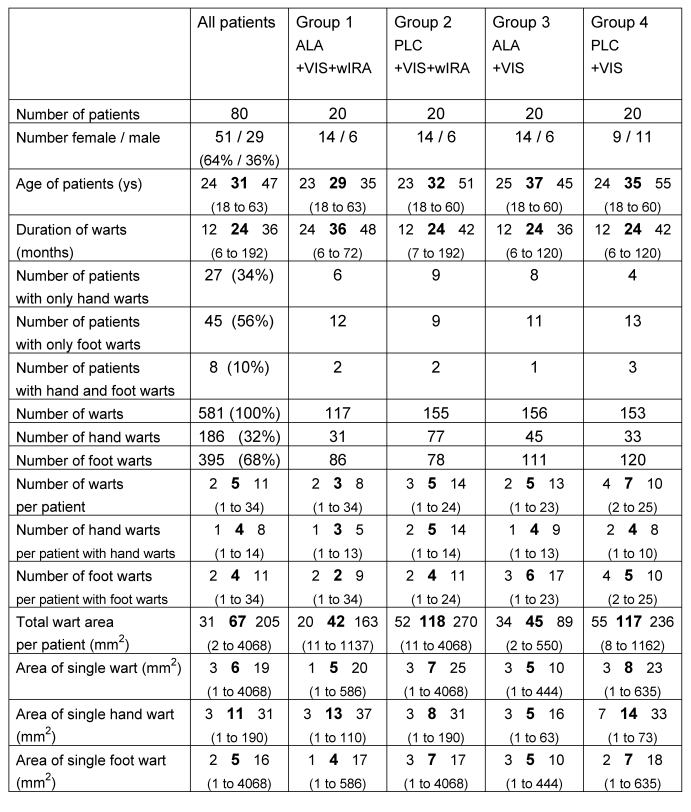
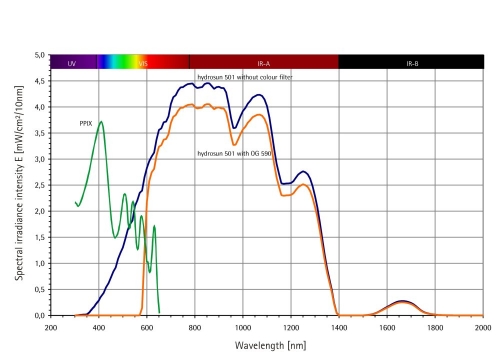
Methods: Pre-treatment with keratolysis (salicylic acid) and curettage. PDT treatment: topical application of 5-ALA (Medac) in "unguentum emulsificans aquosum" vs. placebo; irradiation: combination of VIS and a large amount of wIRA (Hydrosun) radiator type 501, 4 mm water cuvette, waterfiltered spectrum 590-1400 nm, contact-free, typically painless) vs. VIS alone. Post-treatment with retinoic acid ointment. One to three therapy cycles every 3 weeks. Main variable of interest: "Percent change of total wart area of each patient over the time" (18 weeks). Global judgement by patient and by physician and subjective rating of feeling/pain (visual analogue scales). 80 patients with therapy-resistant common hand and foot warts were assigned randomly into one of the four therapy groups with comparable numbers of warts at comparable sites in all groups.
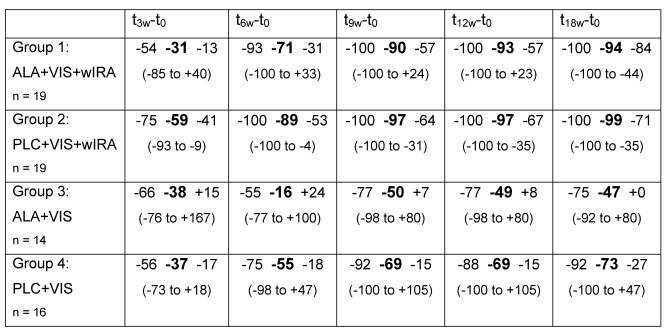
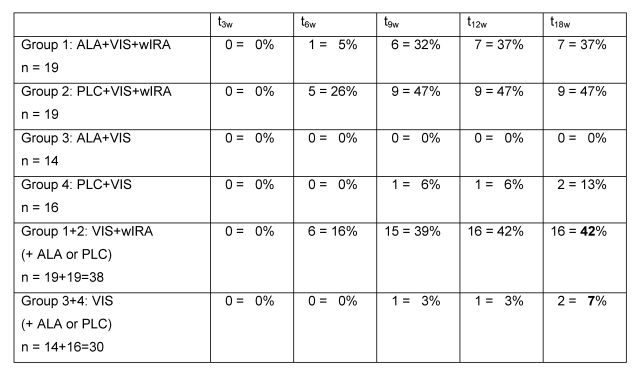
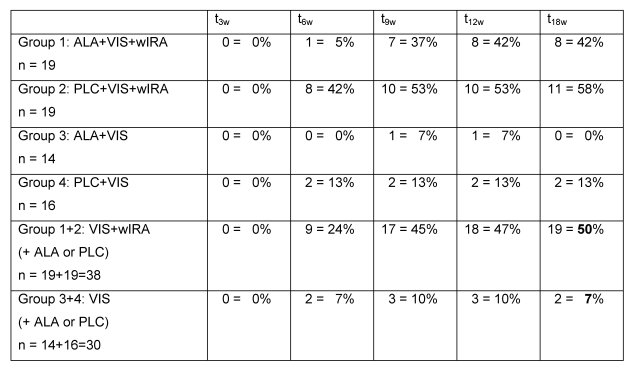
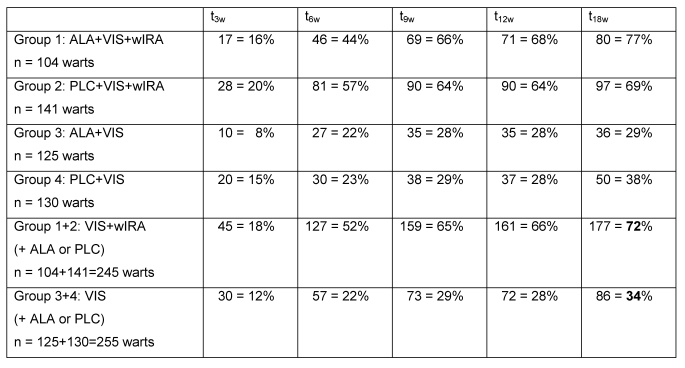
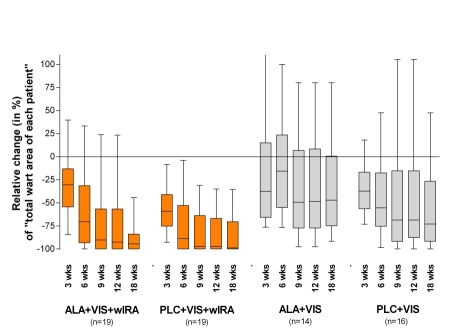
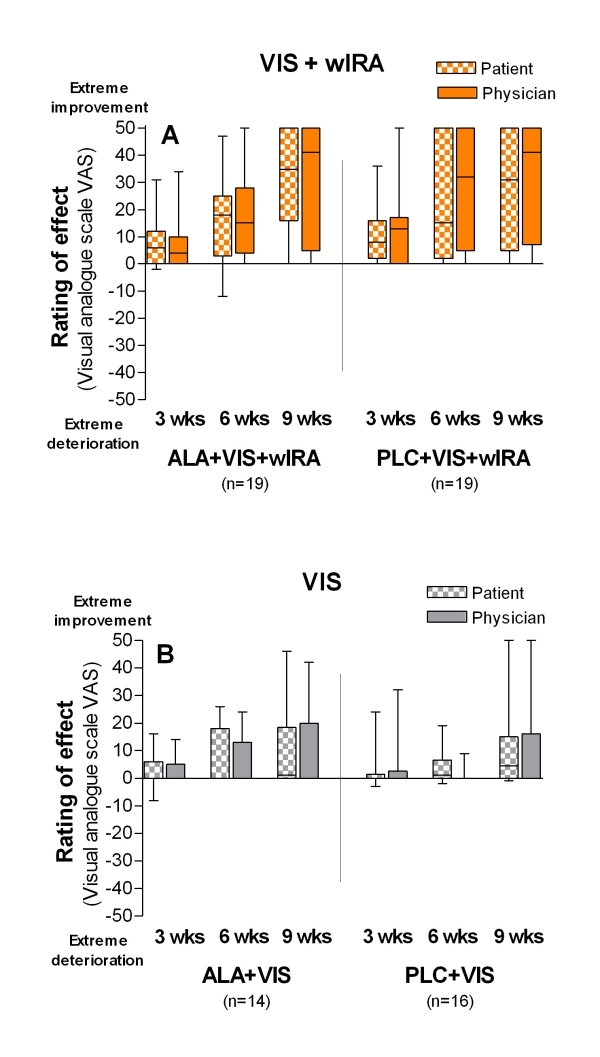
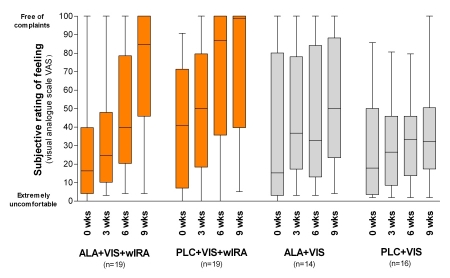
Results: The individual total wart area decreased during 18 weeks in group 1 (ALA+VIS+wIRA) and in group 2 (PLC+VIS+wIRA) significantly more than in both groups without wIRA (group 3 (ALA+VIS) and 4 (PLC+VIS)): medians and interquartile ranges: -94% (-100%/-84%) vs. -99% (-100%/-71%) vs. -47% (-75%/0%) vs. -73% (-92%/-27%). After 18 weeks the two groups with wIRA differed remarkably from the two groups without wIRA: 42% vs. 7% completely cured patients; 72% vs. 34% vanished warts. Global judgement by patient and by physician and subjective rating of feeling was much better in the two groups with wIRA than in the two groups without wIRA.
Conclusions: The above described complete treatment scheme of hand and foot warts (keratolysis, curettage, PDT treatment, irradiation with VIS+wIRA, retinoic acid ointment; three therapy cycles every 3 weeks) proved to be effective. Within this treatment scheme wIRA as non-invasive and painless treatment modality revealed to be an important, effective factor, while photodynamic therapy with 5-ALA in the described form did not contribute recognisably - neither alone (without wIRA) nor in combination with wIRA - to a clinical improvement. For future treatment of warts an even improved scheme is proposed: one treatment cycle (keratolysis, curettage, wIRA, without PDT) once a week for six to nine weeks.
Hintergrund: Vulgäre Warzen (Verrucae vulgares) sind humane Papillomvirus-Infektionen (HPV) mit einer hohen Inzidenz und Prävalenz, die am häufigsten Hände und Füße befallen und die in der Lage sind, die Lebensqualität zu beeinträchtigen. Etwa 30 in der Literatur beschriebene Therapieverfahren zeugen von einem Mangel an einer einzigen überzeugenden Strategie. Jüngste Veröffentlichungen zeigten positive Ergebnisse der Photodynamischen Therapie (PDT) mit 5-Aminolävulinsäure (5-ALA) in der Therapie von HPV-induzierten Hautkrankheiten, besonders Warzen, wobei sichtbares Licht (VIS) verwendet wird, um ein Absorptionsband des endogen aus 5-ALA gebildeten Protoporphyrin IX zu stimulieren. Weitere Erfahrungen, wassergefiltertes Infrarot A (wIRA) während der 5-ALA-PDT zusätzlich anzuwenden, offenbarten positive Wirkungen.
Ziel der Untersuchung: Erste prospektive randomisierte kontrollierte Blind-Studie, die PDT und wIRA in die Behandlung von therapierefraktären vulgären Hand- und Fußwarzen einbezieht.
Vergleich von "5-ALA-Salbe (ALA) vs. Placebo-Salbe (PLC)" und "Bestrahlung mit sichtbarem Licht und wIRA (VIS+wIRA) vs. Bestrahlung mit sichtbarem Licht allein (VIS)".
Methoden: Vorbehandlung mit Keratolyse (Salizylsäure) und Kürettage. Photodynamische Therapie (PDT): topische Applikation von 5-ALA (Medac) in "Unguentum emulsificans aquosum" vs. Placebo; Bestrahlung: Kombination von sichtbarem Licht (VIS) und einem hohen Maß an wassergefiltertem Infrarot A (wIRA) (Hydrosun®-Strahler Typ 501, 4 mm Wasserküvette, wassergefiltertes Spektrum 590-1400 nm, kontaktfrei, typischerweise schmerzlos) vs. sichtbares Licht (VIS) allein. Nachbehandlung mit Vitamin-A-Säure-Salbe. Ein bis drei Therapiezyklen im Abstand von 3 Wochen. Hauptzielvariable: "Prozentuale Änderung der Gesamtwarzenfläche jedes Patienten über die Zeit" (18 Wochen). Globales Urteil von Patient und von Arzt sowie subjektive Einschätzung von Empfindung/Schmerz (visuelle Analogskalen).
80 Patienten mit therapierefraktären vulgären Hand- und Fußwarzen wurden randomisiert einer der vier Behandlungsgruppen (mit vergleichbarer Anzahl an Warzen in vergleichbaren Lokalisationen in allen Gruppen) zugeteilt.
Ergebnisse: Die individuelle Gesamtwarzenfläche nahm während 18 Wochen in Gruppe 1 (ALA+VIS+wIRA) und in Gruppe 2 (PLC+VIS+wIRA) signifikant mehr als in den beiden Gruppen ohne wIRA (Gruppe 3 (ALA+VIS) und 4 (PLC+VIS)) ab: Mediane und Interquartil-Spannen:
-94% (-100%/-84%) vs. -99% (-100%/-71%) vs. -47% (-75%/0%) vs. -73% (-92%/-27%).
Nach 18 Wochen unterschieden sich die zwei Gruppen mit wIRA deutlich von den zwei Gruppen ohne wIRA: 42% vs. 7% komplett geheilte Patienten; 72% vs. 34% völlig verschwundene Warzen.
Das globale Urteil von Patient und von Arzt und die subjektive Einschätzung des Empfindens waren in den zwei Gruppen mit wIRA viel besser als in den zwei Gruppen ohne wIRA.
Folgerungen: Das oben beschriebene vollständige Therapieschema von Hand- und Fußwarzen (Keratolyse, Kürettage, Photodynamische Therapie, Bestrahlung mit VIS+wIRA, Vitamin-A-Säure-Salbe; drei Therapiezyklen im Abstand von 3 Wochen) erwies sich als effektiv. Innerhalb des Therapieschemas zeigte sich wIRA - als nicht-invasive und schmerzlose Therapiemodalität - als ein wichtiger, effektiver Faktor, während die Photodynamische Therapie mit 5-ALA in der beschriebenen Form nicht erkennbar - weder alleine (ohne wIRA) noch in Kombination mit wIRA - zu einer klinischen Verbesserung beitrug.
Für die zukünftige Behandlung von Warzen wird ein weiter verbessertes Schema vorgeschlagen: ein Therapiezyklus (Keratolyse, Kürettage, wIRA, ohne PDT) einmal pro Woche für sechs bis neun Wochen.
Keywords: 5-aminolevulinic acid (5-ALA); human papilloma virus (HPV); photodynamic therapy (PDT); warts; waterfiltered infrared A (wIRA).
Figures
References
-
- Sterling J, Kurtz JB. Viral infections. In: Champion RH, Burton JL, Burns DA, Breathnach SM, editors. Rook/Wilkinson/Ebling textbook of dermatology. 6th ed. Oxford: Blackwell Scientific; 1998. pp. 995–1095.
-
- Combemale P, Delolme H, Dupin M. Traitment des verrues. Ann Dermatol Venereol. 1998;125(6-7):443–462. - PubMed
-
- Sterling JC, Handfield-Jones S, Hudson PM British Association of Dermatologists. Guidelines for the management of cutaneous warts. Br J Dermatol. 2001;144(1):4–11. - PubMed
-
- Kalka K, Merk H, Mukhtar H. Photodynamic therapy in dermatology. J Am Acad Dermatol. 2000;42(3):389–413. quiz 414-6. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials