

Management of fibromyalgia syndrome--an interdisciplinary evidence-based guideline
- PMID: 19675740
- PMCID: PMC2703259
Management of fibromyalgia syndrome--an interdisciplinary evidence-based guideline
Abstract
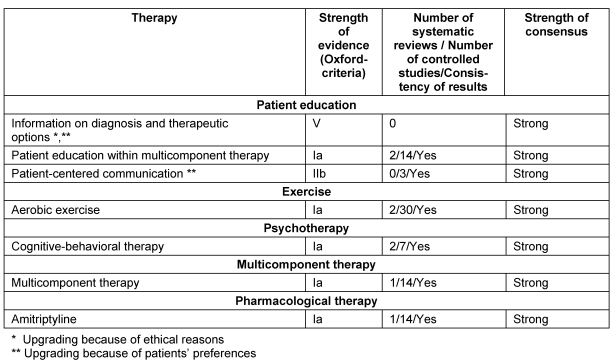
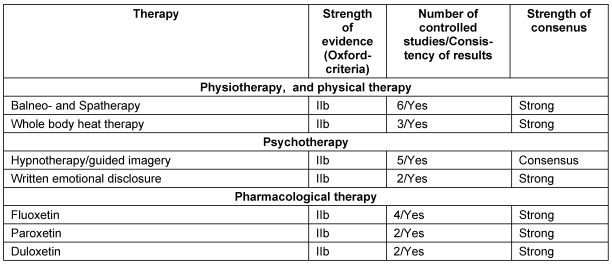
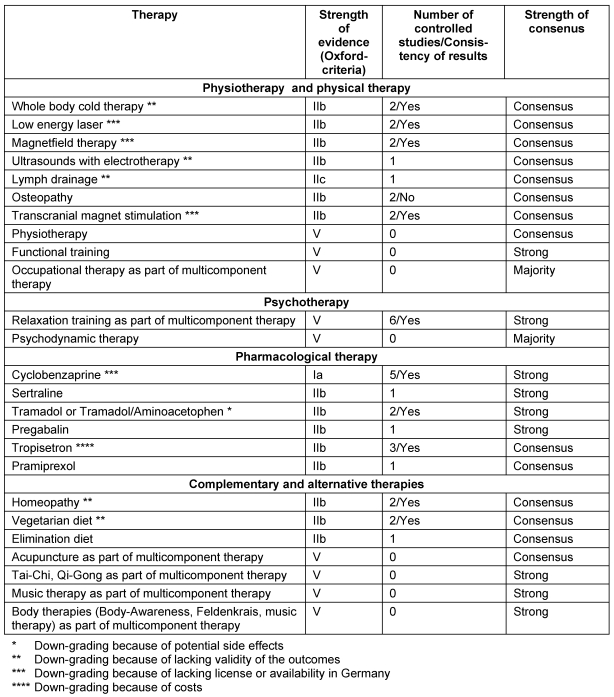
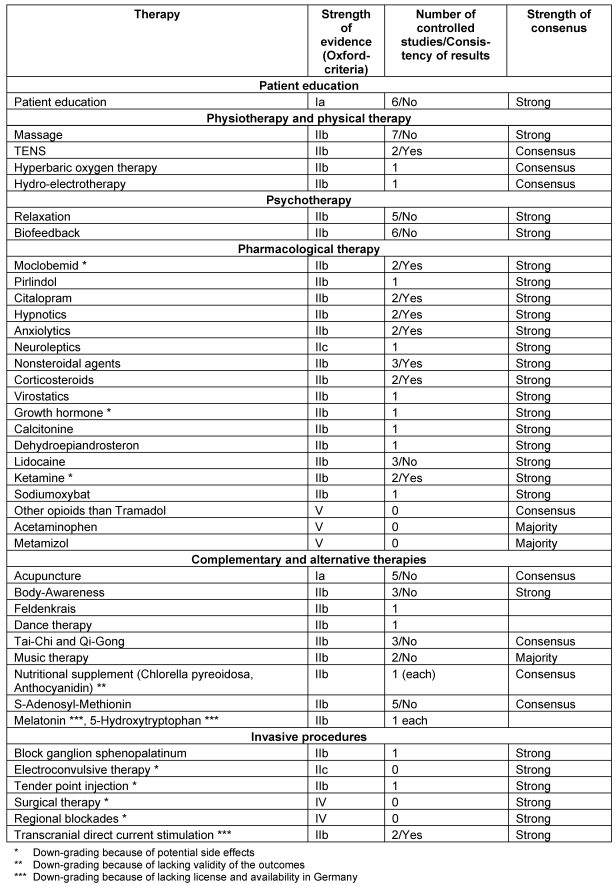
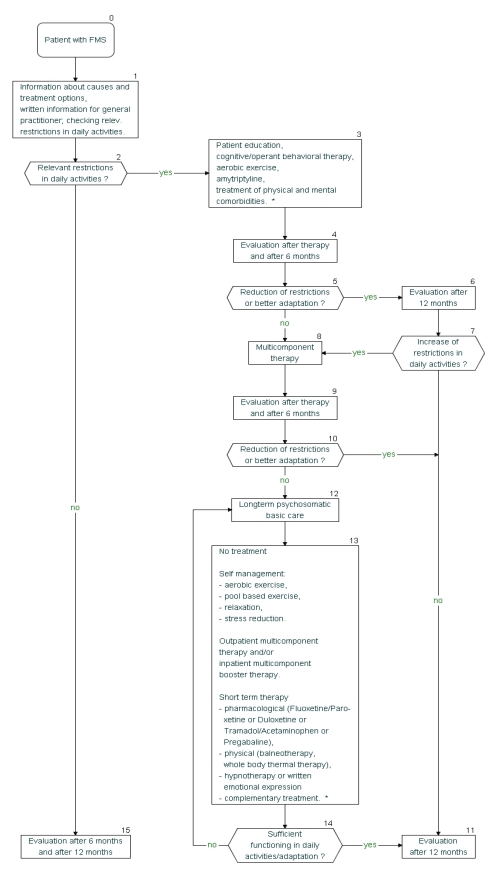
The prevalence of fibromyalgia syndrome (FMS) of 1-2% in the general population associated with high disease-related costs and the conflicting data on treatment effectiveness had led to the development of evidence-based guidelines designed to provide patients and physicians guidance in selecting among the alternatives. Until now no evidence-based interdisciplinary (including patients) guideline for the management of FMS was available in Europe. Therefore a guideline for the management of fibromyalgia syndrome (FMS) was developed by 13 German medical and psychological associations and two patient self-help organisations. The task was coordinated by two German scientific umbrella organisations, the Association of the Scientific Medical Societies in Germany AWMF and the German Interdisciplinary Association of Pain Therapy DIVS. A systematic search of the literature including all controlled studies, systematic reviews and meta-analyses of pharmacological and non-pharmacological treatments of FMS was performed in the Cochrane Library (1993-12/2006), Medline (1980-12/2006), PsychInfo (1966-12/2006) and Scopus (1980-12/ 2006). Levels of evidence were assigned according to the classification system of the Oxford-Centre for Evidence Based Medicine. Grading of the strengths of recommendations was done according to the German program for disease management guidelines. Standardized procedures were used to reach a consensus on recommendations. The guideline was reviewed and finally approved by the boards of the societies involved and published online by the AWMF on april 25, 2008: http://www.uni-duesseldorf.de/AWMF/ll/041-004.htm. A short version of the guideline for patients is available as well: http://www.uni-duesseldorf.de/AWMF/ll/041-004p.htm. The following procedures in the management of fms were strongly recommended: information on diagnosis and therapeutic options and patient-centered communication, aerobic exercise, cognitive and operant behavioural therapy, multicomponent treatment and amitriptyline. Based on expert opinion, a stepwise FMS-management was proposed. Step 1 comprises confirming the diagnosis and patient education and treatment of physical or mental comorbidities or aerobic exercise or cognitive behavioural therapy or amitriptyline. Step 2 includes multicomponent treatment. Step 3 comprises no further treatment or self-management (aerobic exercise, stress management) and/or booster multicomponent therapy and/or pharmacological therapy (duloxetine or fluoxetine or paroxetine or pregabalin or tramadol/aminoacetophen) and/or psychotherapy (hypnotherapy or written emotional disclosure) and/or physical therapy (balneotherapy or whole body heat therapy) and/or complementary therapies (homeopathy or vegetarian diet). The choice of treatment options should be based on informed decision-making and respect of the patients' preferences.
Die Prävalenz des Fibromyalgiesyndroms (FMS) in der allgemeinen Bevölkerung beträgt 1–2%. Aufgrund der mit FMS verbundenen hohen Krankheitskosten und den widersprüchlichen Daten zur Wirksamkeit einzelner Behandlungsformen wurden evidenzbasierte Leitlinien entwickelt, um Ärzten und Patienten einen Entscheidungshilfe zu geben. Bisher war in Europa keine interdisziplinäre evidenzbasierte Leitlinie unter Einschluss von Patienten zum FMS verfügbar.
Deswegen wurde von 13 deutschen medizinischen und psychologischen Fachgesellschaften und zwei Patientenselbsthilfeorganisationen eine Leitlinie zu Therapie des FMS entwickelt. Die Durchführung wurde von der Deutschen Interdisziplinären Vereinigung für Schmerztherapie DIVS und der Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften in Deutschland AWMF koordiniert. Eine systematische Literatursuche aller kontrollierte Studien, systematischer Reviews und Metaanalysen wurde über die Datenbanken Cochrane Library (1993–12/2006), Medline (1980–12/2006), PsychInfo (1966–12/2006) und Scopus (1980–12/ 2006) durchgeführt. Für die Vergabe von Evidenzklassen wurde das System des Oxford-Centre for Evidence Based Medicine verwendet. Für die Vergabe von Empfehlungsgraden wurde die Empfehlungsgraduierung der nationalen Versorgungsleitlinien verwendet. Die Erstellung der Empfehlungen erfolgte in einem mehrstufigen nominalen Gruppenprozess, welcher von einer Vertreterin der AWMF moderiert wurde. Die Leitlinie wurde von den Vorständen der beteiligten Fachgesellschaften begutachtet und genehmigt. Die wissenschaftliche Lang- und Kurzversion der Leitlinie wurde am 25. April 2008 von der AWMF ins Internet gestellt:
Folgende Therapieverfahren erhielten eine starke Empfehlung: Informationen über Diagnose und Behandlungsmöglichkeiten, patienten-zentrierte Kommunikation, aerobes Ausdauertraining, kognitive und operante Verhaltenstherapie, multimodale Therapie und Amitriptylin. Basierend auf Expertenmeinung wurde eine stufenweise Behandlung des FMS empfohlen: Stufe 1 beinhaltet Diagnosebestätigung und Patientenschulung und/oder Behandlung körperlicher und psychischer Komorbiditäten oder aerobes Ausdauertraining oder kognitive und operante Verhaltenstherapie oder Amitriptylin. Stufe 2 beinhaltet multimodale Therapie. Stufe 3 umfasst die folgenden Behandlungsoptionen: keine weitere Behandlung oder Selbstmanagement (aerobes Ausdauertraining, Stressmanagement) und/oder multimodale Auffrischungstherapie und/oder phamakologische Therapie (Duloxetin oder Fluoxetin oder Pregabalin oder Tramadol/Paracetamol) und/oder psychotherapeutische Verfahren (Hypnotherapie oder therapeutisches Schreiben) oder physikalische Therapie (Balneotherapie oder Ganzkörperwärmetherapie) und/oder komplementäre Therapien (Homöopathie oder vegetarische Kost). Die Wahl der Behandlungsoptionen soll auf gemeinsame Entscheidungsfindung und unter Berücksichtigung der Patientenpräferenzen durchgeführt werden.
Keywords: fibromyalgia syndrome; guideline; management; systematic review.
Figures
References
-
- Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, Tugwell P, Campbell SM, Abeles M, Clark P, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33(2):160–172. DOI: 10.1002/art.1780330203. Available from: http://dx.doi.org/10.1002/art.1780330203. - DOI - PubMed
-
- Croft PR. The epidemiology of chronic widespread pain. J Musculoskel Pain. 2002;10(1-2):1–199.
-
- Henningsen P, Zimmermann T, Sattel H. Medically unexplained physical symptoms, anxiety, and depression: a meta-analytic review. Psychosom Med. 2003;65(4):528–533. DOI: 10.1097/01.PSY.0000075977.90337.E7. Available from: http://dx.doi.org/10.1097/01.PSY.0000075977.90337.E7. - DOI - PubMed
-
- Van Houdenhove B, Luyten P. Stress, depression and fibromyalgia. Acta Neurol Belg. 2006;106(4):149–156. - PubMed
-
- Wolfe F, Anderson J, Harkness D, Bennett RM, Caro XJ, Goldenberg DL, Russell IJ, Yunus MB. A prospective, longitudinal, multicenter study of service utilization and costs in fibromyalgia. Arthritis Rheum. 1997;40(9):1560–1570. DOI: 10.1002/art.1780400904. Available from: http://dx.doi.org/10.1002/art.1780400904. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous