

Coffee intake is associated with lower rates of liver disease progression in chronic hepatitis C
- PMID: 19676128
- PMCID: PMC2783828
- DOI: 10.1002/hep.23162
Coffee intake is associated with lower rates of liver disease progression in chronic hepatitis C
Abstract
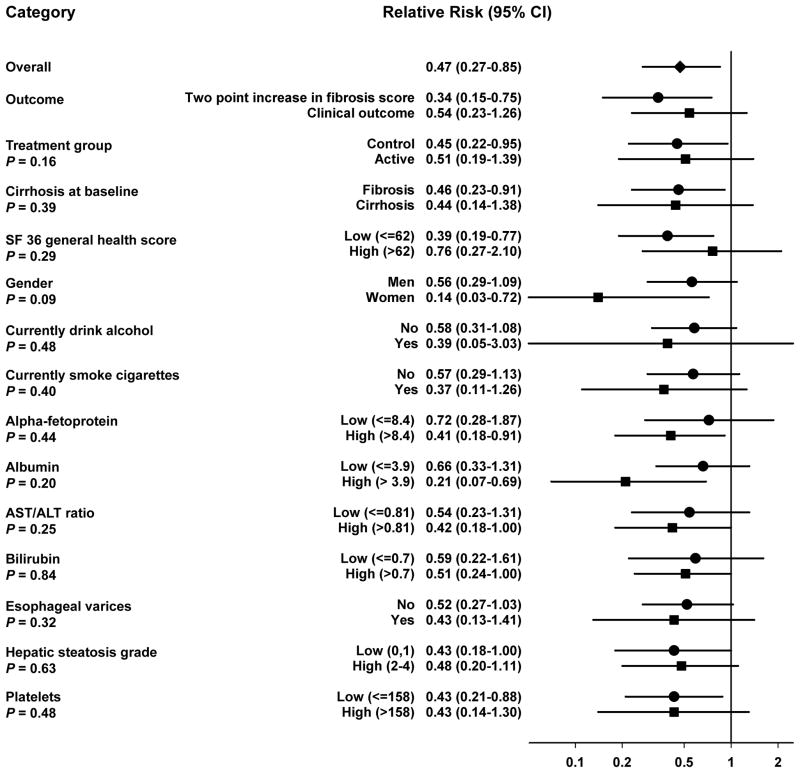
Higher coffee consumption has been associated inversely with the incidence of chronic liver disease in population studies. We examined the relationship of coffee consumption with liver disease progression in individuals with advanced hepatitis C-related liver disease. Baseline coffee and tea intake were assessed in 766 participants of the Hepatitis C Antiviral Long-Term Treatment against Cirrhosis (HALT-C) trial who had hepatitis C-related bridging fibrosis or cirrhosis on liver biopsy and failed to achieve a sustained virological response to peginterferon plus ribavirin treatment. Participants were followed for 3.8 years for clinical outcomes and, for those without cirrhosis, a 2-point increase in Ishak fibrosis score on protocol biopsies. At baseline, higher coffee consumption was associated with less severe steatosis on biopsy, lower serum aspartate aminotransferase (AST)/alanine aminotransferase (ALT) ratio, alpha-fetoprotein, insulin, and homeostatic model assessment (HOMA2) score, and higher albumin (P < 0.05 for all). Two hundred thirty patients had outcomes. Outcome rates declined with increasing coffee intake: 11.1/100 person-years for none, 12.1 for less than 1 cup/day, 8.2 for 1 to fewer than 3 cups/day, and 6.3 for 3 or more cups/day (P-trend = 0.0011). Relative risks (95% confidence intervals) were 1.11 (0.76-1.61) for less than 1 cup/day; 0.70 (0.48-1.02) for 1 to fewer than 3 cups/day; and 0.47 (0.27-0.85) for 3 or more cups/day (P-trend = 0.0003) versus not drinking. Risk estimates did not vary by treatment assignment or cirrhosis status at baseline. Tea intake was not associated with outcomes.
Conclusion: In a large prospective study of participants with advanced hepatitis C-related liver disease, regular coffee consumption was associated with lower rates of disease progression.
Trial registration: ClinicalTrials.gov NCT00006164.
Figures
Comment in
-
Coffee intake and chronic hepatitis C.Hepatology. 2009 Nov;50(5):1673; author reply 1673. doi: 10.1002/hep.23243. Hepatology. 2009. PMID: 19876946 No abstract available.
-
Tea intake and liver diseases.Hepatology. 2011 Jan;53(1):373-4. doi: 10.1002/hep.23872. Epub 2010 Jul 29. Hepatology. 2011. PMID: 20890888 No abstract available.
-
Coffee and progression of liver disease.Natl Med J India. 2010 Mar-Apr;23(2):91-3. Natl Med J India. 2010. PMID: 20925207 No abstract available.
References
-
- Williams R. Global challenges in liver disease. Hepatology. 2006;44:521–526. - PubMed
-
- Fried MW, Shiffman ML, Reddy KR, Smith C, Marinos G, Goncales FL, Jr, et al. Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. N Engl J Med. 2002;347:975–982. - PubMed
-
- Arnesen E, Huseby NE, Brenn T, Try K. The Tromso Heart Study: distribution of, and determinants for, gamma-glutamyltransferase in a free-living population. Scand J Clin Lab Invest. 1986;46:63–70. - PubMed
-
- Casiglia E, Spolaore P, Ginocchio G, Ambrosio GB. Unexpected effects of coffee consumption on liver enzymes. Eur J Epidemiol. 1993;9:293–297. - PubMed
-
- Honjo S, Kono S, Coleman MP, Shinchi K, Sakurai Y, Todoroki I, et al. Coffee consumption and serum aminotransferases in middle-aged Japanese men. J Clin Epidemiol. 2001;54:823–829. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- N01-DK-9-2325/DK/NIDDK NIH HHS/United States
- M01RR-00042/RR/NCRR NIH HHS/United States
- M01RR-00051/RR/NCRR NIH HHS/United States
- N01-DK-9-2321/DK/NIDDK NIH HHS/United States
- N01-DK-9-2320/DK/NIDDK NIH HHS/United States
- M01 RR006192/RR/NCRR NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- M01 RR000065/RR/NCRR NIH HHS/United States
- N01-DK-9-2322/DK/NIDDK NIH HHS/United States
- M01 RR000043/RR/NCRR NIH HHS/United States
- N01-DK-9-2323/DK/NIDDK NIH HHS/United States
- M01 RR000042/RR/NCRR NIH HHS/United States
- M01 RR000827/RR/NCRR NIH HHS/United States
- M01RR-00065/RR/NCRR NIH HHS/United States
- N01-DK-9-2328/DK/NIDDK NIH HHS/United States
- N01-DK-9-2318/DK/NIDDK NIH HHS/United States
- N01-DK-9-2324/DK/NIDDK NIH HHS/United States
- N01-DK-9-2319/DK/NIDDK NIH HHS/United States
- M01RR-00827/RR/NCRR NIH HHS/United States
- N01-DK-9-2327/DK/NIDDK NIH HHS/United States
- M01RR-01066/RR/NCRR NIH HHS/United States
- N01 DK092326/DK/NIDDK NIH HHS/United States
- M01 RR000633/RR/NCRR NIH HHS/United States
- M01 RR000051/RR/NCRR NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- N01-DK-9-2326/DK/NIDDK NIH HHS/United States
- M01RR-00633/RR/NCRR NIH HHS/United States
- M01RR-00043/RR/NCRR NIH HHS/United States
- M01RR-06192/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases