

Primary care-based multifaceted, interdisciplinary medical educational intervention for patients with systolic heart failure: lessons learned from a cluster randomised controlled trial
- PMID: 19678944
- PMCID: PMC2736948
- DOI: 10.1186/1745-6215-10-68
Primary care-based multifaceted, interdisciplinary medical educational intervention for patients with systolic heart failure: lessons learned from a cluster randomised controlled trial
Abstract
Background: Chronic (systolic) heart failure (CHF) is a common and disabling condition. Adherence to evidence-based guidelines in primary care has been shown to improve health outcomes. The aim was to explore the impact of a multidisciplinary educational intervention for general practitioners (GPs) (Train the trainer = TTT) on patient and performance outcomes.
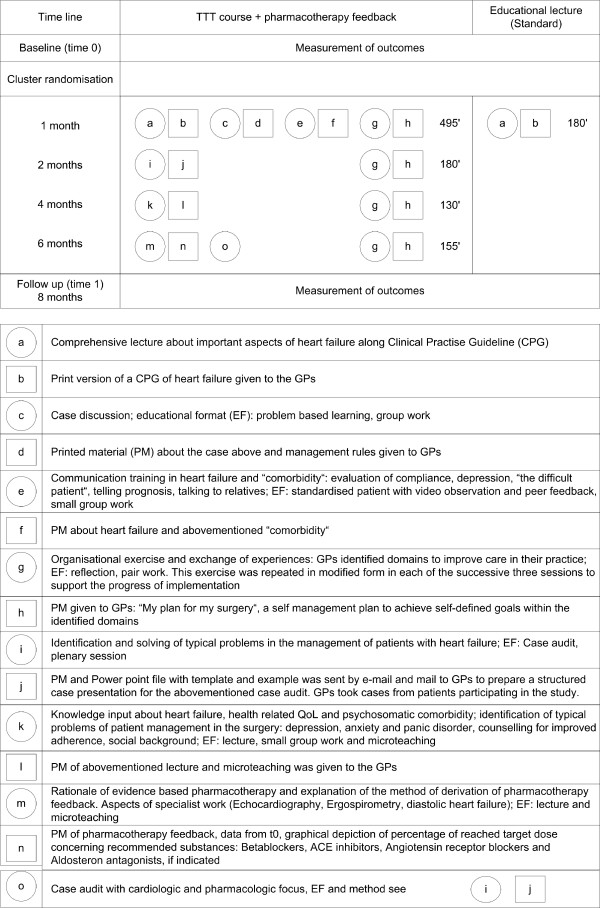
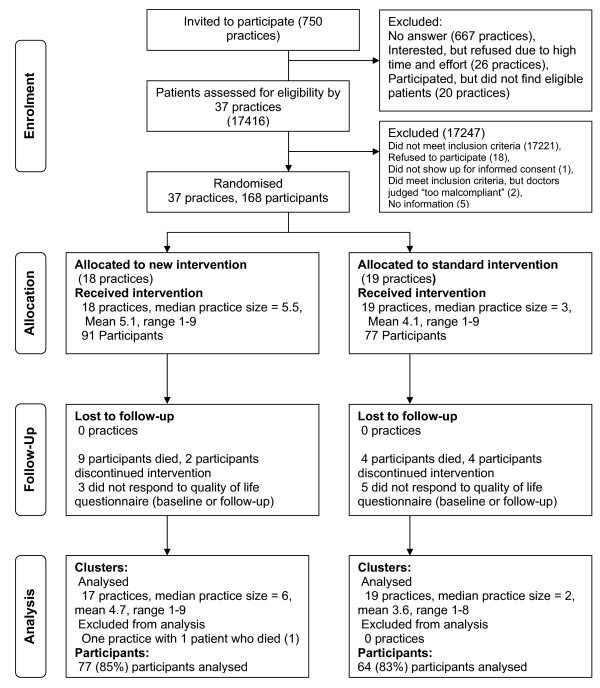
Methods: This paper presents the key findings from the trial and discusses the lessons learned during the implementation of the TTT trial. Primary care practices were randomly assigned to the TTT intervention or to the control group. 37 GPs (18 TTT, 19 control) were randomised and 168 patients diagnosed with ascertained CHF (91 TTT, 77 control) were enrolled. GPs in the intervention group attended four meetings addressing clinical practice guidelines and pharmacotherapy feedback. The primary outcome was patient self-reported quality of life at seven months, using the SF-36 Physical Functioning scale. Secondary outcomes included other SF-36 scales, the Kansas City Cardiomyopathy Questionnaire (KCCQ), total mortality, heart failure hospital admissions, prescribing, depressive disorders (PHQ-9), behavioural change (European Heart Failure Self-Care Behaviour Scale), patient-perceived quality of care (EUROPEP) and improvement of heart failure using NT-proBNP-levels. Because recruitment targets were not achieved an exploratory analysis was conducted.
Results: There was high baseline achievement in both groups for many outcomes. At seven months, there were no significant mean difference between groups for the primary outcome measure (-3.3, 95%CI -9.7 to 3.1, p = 0.30). The only difference in secondary outcomes related to the prescribing of aldosterone antagonists by GPs in the intervention group, with significant between group differences at follow-up (42 vs. 24%, adjusted OR = 4.0, 95%CI 1.2-13; p = 0.02).
Conclusion: The intervention did not change the primary outcome or most secondary outcomes. Recruitment targets were not achieved and the under-recruitment of practices and patients alongside a selection bias of participating GPs, prohibit definite conclusions, but the CI indicates a non-effectiveness of the intervention in this sample. We describe the lessons learned from conducting the trial for the future planning and conduct of confirmatory trials in primary care.
Trial registration: ISRCTN08601529.
Figures
References
-
- Swedberg K, Cleland J, Dargie H, Drexler H, Follath F, Komajda M, Tavazzi L, Smiseth OA, Gavazzi A, Haverich A, Hoes A, Jaarsma T, Korewicki J, Lévy S, Linde C, Lopez-Sendon JL, Nieminen MS, Piérard L, Remme WJ, Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology Guidelines for the diagnosis and treatment of chronic heart failure: executive summary (update 2005): The Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology. Eur Heart J. 2005;26:1115–1140. doi: 10.1093/eurheartj/ehi166. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
