

Outcome of extracorporeal membrane oxygenation for early primary graft failure after pediatric heart transplantation
- PMID: 19679252
- PMCID: PMC3117294
- DOI: 10.1016/j.jacc.2009.04.062
Outcome of extracorporeal membrane oxygenation for early primary graft failure after pediatric heart transplantation
Abstract
Objectives: We sought to analyze the indications and outcome of extracorporeal membrane oxygenation (ECMO) for early primary graft failure and determine its impact on long-term graft function and rejection risk.
Background: Early post-operative graft failure requiring ECMO can complicate heart transplantation.
Methods: A retrospective review of all children requiring ECMO in the early period after transplantation from 1990 to 2007 was undertaken.
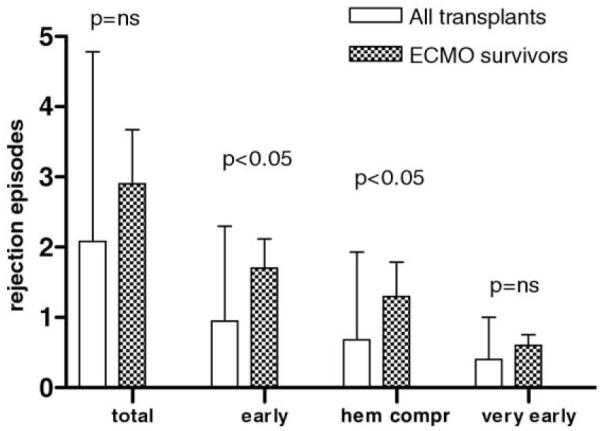
Results: Twenty-eight (9%) of 310 children who underwent transplantation for cardiomyopathy (n = 5) or congenital heart disease (n = 23) required ECMO support. The total ischemic time was significantly longer for ECMO-rescued recipients compared with our overall transplantation population (276 +/- 86 min vs. 242 +/- 70 min, p < 0.01). The indication for transplantation, for ECMO support, and the timing of cannulation had no impact on survival. Hyperacute rejection was uncommon. Fifteen children were successfully weaned off ECMO and discharged alive (54%). Mean duration of ECMO was 2.8 days for survivors (median 3 days) compared with 4.8 days for nonsurvivors (median 5 days). There was 100% 3-year survival in the ECMO survivor group, with 13 patients (46%) currently alive at a mean follow-up of 8.1 +/- 3.8 years. The graft function was preserved (shortening fraction 36 +/- 7%), despite an increased number of early rejection episodes (1.7 +/- 1.6 vs. 0.7 +/- 1.3, overall transplant population, p < 0.05) and hemodynamically comprising rejection episodes (1.3 +/- 1.9 vs. 0.7 +/- 1.3, overall transplant population, p < 0.05).
Conclusions: Overall survival was 54%, with all patients surviving to at least 3 years after undergoing transplantation. None of the children requiring >4 days of ECMO support survived. Despite an increased number of early and hemodynamically compromising rejections, the long-term graft function is similar to our overall transplantation population.
Figures


Comment in
-
Re: Outcome of extracorporeal membrane oxygenation for early primary graft failure after pediatric heart transplantation.J Am Coll Cardiol. 2009 Aug 18;54(8):738-9. doi: 10.1016/j.jacc.2009.05.026. J Am Coll Cardiol. 2009. PMID: 19679253 No abstract available.
References
-
- Kirk R, Edwards LB, Aurora P, et al. Registry of the International Society for Heart and Lung Transplantation: eleventh official pediatric heart transplantation report—2008. J Heart Lung Transplant. 2008;27:970–7. - PubMed
-
- Canter C, Naftel D, Caldwell R, et al. Survival and risk factors for death after cardiac transplantation in infants. A multi-institutional study. The Pediatric Heart Transplant Study. Circulation. 1997;96:227–31. - PubMed
-
- Goland S, Czer LS, Kass RM, et al. Pre-existing pulmonary hypertension in patients with end-stage heart failure: impact on clinical outcome and hemodynamic follow-up after orthotopic heart transplantation. J Heart Lung Transplant. 2007;26:312–8. - PubMed
-
- Kanter KR, Pennington G, Weber TR, Zambie MA, Braun P, Martychenko V. Extracorporeal membrane oxygenation for postoperative cardiac support in children. J Thorac Cardiovasc Surg. 1987;93:27–35. - PubMed
-
- Kanter KR, Pennington DG, McBride LR, et al. Mechanical circulatory assistance after heart transplantation. J Heart Transplant. 1987;6:150–4. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
