

Contrast-enhanced anatomic imaging as compared to contrast-enhanced tissue characterization for detection of left ventricular thrombus
- PMID: 19679285
- PMCID: PMC5057386
- DOI: 10.1016/j.jcmg.2009.03.017
Contrast-enhanced anatomic imaging as compared to contrast-enhanced tissue characterization for detection of left ventricular thrombus
Abstract
Objectives: This study sought to compare contrast-enhanced anatomic imaging and contrast-enhanced tissue characterization (delayed-enhancement cardiac magnetic resonance [DE-CMR]) for left ventricular (LV) thrombus detection.
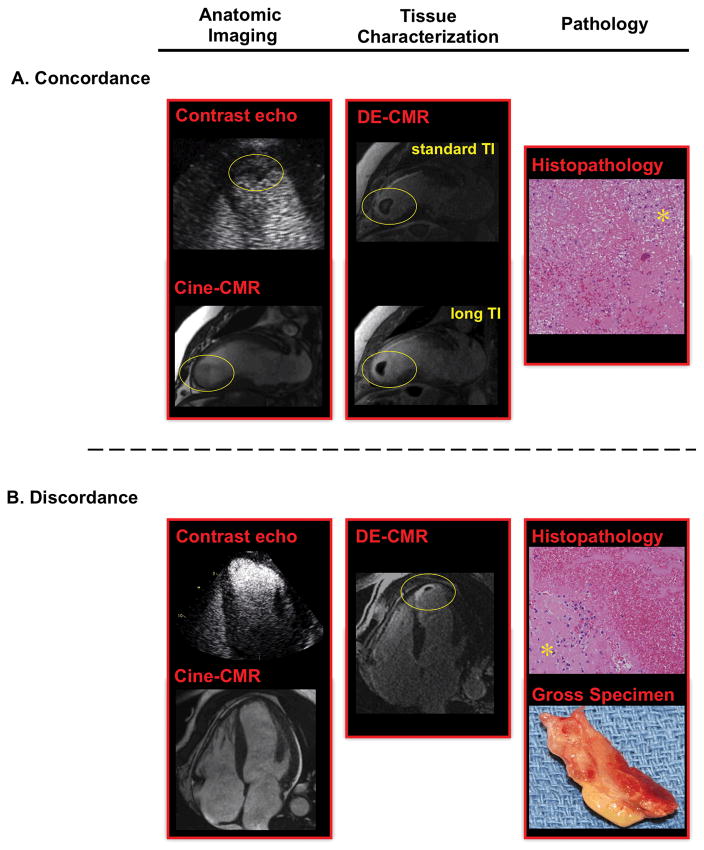
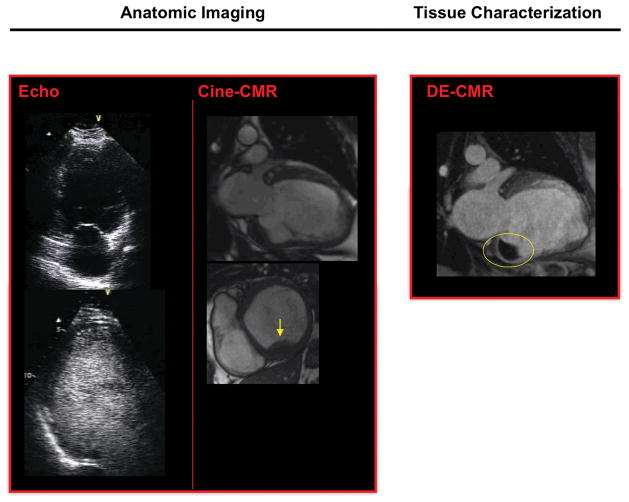
Background: Contrast echocardiography (echo) detects LV thrombus based on anatomic appearance, whereas DE-CMR imaging detects thrombus based on tissue characteristics. Although DE-CMR has been validated as an accurate technique for thrombus, its utility compared with contrast echo is unknown.
Methods: Multimodality imaging was performed in 121 patients at high risk for thrombus due to myocardial infarction or heart failure. Imaging included 3 anatomic imaging techniques for thrombus detection (contrast echo, noncontrast echo, cine-CMR) and a reference of DE-CMR tissue characterization. LV structural parameters were quantified to identify markers for thrombus and predictors of additive utility of contrast-enhanced thrombus imaging.
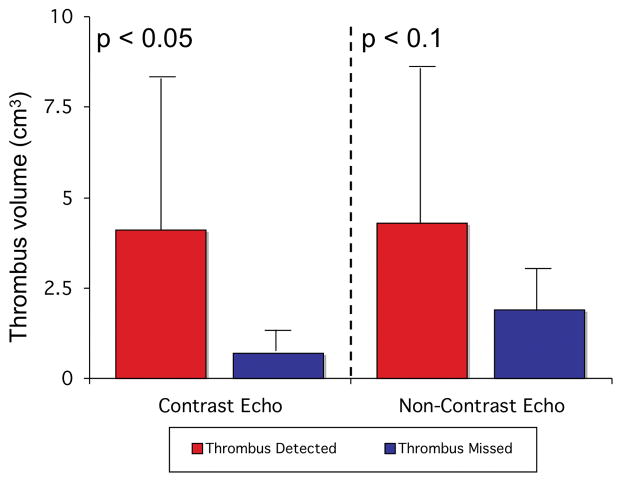
Results: Twenty-four patients had thrombus by DE-CMR. Patients with thrombus had larger infarcts (by DE-CMR), more aneurysms, and lower LV ejection fraction (by CMR and echo) than those without thrombus. Contrast echo nearly doubled sensitivity (61% vs. 33%, p < 0.05) and yielded improved accuracy (92% vs. 82%, p < 0.01) versus noncontrast echo. Patients who derived incremental diagnostic utility from DE-CMR had lower LV ejection fraction versus those in whom noncontrast echo alone accurately assessed thrombus (35 +/- 9% vs. 42 +/- 14%, p < 0.01), with a similar trend for patients who derived incremental benefit from contrast echo (p = 0.08). Contrast echo and cine-CMR closely agreed on the diagnosis of thrombus (kappa = 0.79, p < 0.001). Thrombus prevalence was lower by contrast echo than DE-CMR (p < 0.05). Thrombus detected by DE-CMR but not by contrast echo was more likely to be mural in shape or, when apical, small in volume (p < 0.05).
Conclusions: Echo contrast in high-risk patients markedly improves detection of LV thrombus, but does not detect a substantial number of thrombi identified by DE-CMR tissue characterization. Thrombi detected by DE-CMR but not by contrast echo are typically mural in shape or small in volume.
Conflict of interest statement
This work was partially supported by Lantheus Medical Imaging (echo contrast manufacturer).
Figures
References
-
- Weinsaft J, Kim H, Shah DJ, et al. Detection of Left Ventricular Thrombus by Delayed-Enhancement CMR: Prevalence and Markers in Patients with Systolic Dysfunction. J Am Coll Cardiol. 2008;52:148–57. - PubMed
-
- Srichai MB, Junor C, Rodriguez LL, et al. Clinical, imaging, and pathologic characteristics of left ventricular thrombus: A comparison of contrast enhanced magnetic resonance imaging, transthoracic echocardiography and transesophageal echocardiography with surgical or pathological validation. American Heart Journal. 2006;152:75–84. - PubMed
-
- Mollet NR, Dymarkowski S, Volders W, et al. Visualization of ventricular thrombi with contrast-enhanced magnetic resonance imaging in patients with ischemic heart disease. Circulation. 2002;106:2873–6. - PubMed
-
- Thanigaraj S, Schechtman KB, Perez JE. Improved echocardiographic delineation of left ventricular thrombus with the use of intravenous second-generation contrast image enhancement. J Am Soc Echocardiogr. 1999;12:1022–6. - PubMed
-
- Lang RM, Biereg M, Devereux RM, et al. Recommendations for Chamber Quantification: A Report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, Developed in Conjunction with the European Association of Echocardiography, a Branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18:1440–1463. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
