

Effective testosterone suppression for prostate cancer: is there a best castration therapy?
- PMID: 19680526
- PMCID: PMC2725306
Effective testosterone suppression for prostate cancer: is there a best castration therapy?
Abstract
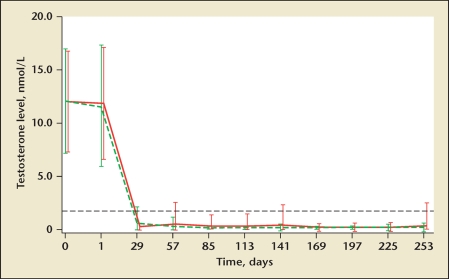
Achieving and maintaining effective suppression of serum testosterone levels in men treated with androgen ablation is one of the essential strategies in the management of prostate cancer. Historically, a serum testosterone below 50 ng/dL was considered to be the castrate level. Current data suggest that the new target for either surgical or chemical castration is a serum testosterone level of lower than 20 ng/dL in an attempt to maximize therapeutic outcomes. Testosterone breakthrough and the acute-on-chronic effects of administration of a luteinizing hormone-releasing hormone analogue may cause testosterone levels to periodically rise, sometimes to noncastrate levels. The goal of androgen ablation is to identify those agents that will most consistently achieve and maintain the lowest testosterone levels possible.
Keywords: Androgen ablation; LHRH analogues; LHRH antagonists; Prostate cancer; Testosterone.
Figures
References
-
- Loblaw DA, Virgo KS, Nam R, et al. Initial hormonal management of androgen-sensitive metastatic, recurrent, or progressive prostate cancer: 2006 update of an American Society of Clinical Oncology practice guideline. J Clin Oncol. 2007;25:1596–1605. - PubMed
-
- [Accessed June 4, 2009];Prostate Cancer V.2.2009. National Comprehensive Cancer Network Web site. http://www.nccn.org/professionals/physician_gls/PDF/prostate.pdf. Registration required.
-
- Tunn U. The current status of intermittent androgen deprivation (IAD) therapy for prostate cancer: putting IAD under the spotlight. BJU Int. 2007;99(suppl 1):19–22. discussion 23–24. - PubMed
-
- Hussain M, Tangen CM, Higano C, et al. Absolute prostate-specific antigen value after androgen deprivation is a strong independent predictor of survival in new metastatic prostate cancer: data from Southwest Oncology Group Trial 9346 (INT-0162) J Clin Oncol. 2006;24:3984–3990. - PubMed
-
- Schulman CC. Hormone therapy for prostate cancer: less is more? Introduction and conclusions. Eur Urol Suppl. 2008;7:743–746.
LinkOut - more resources
Full Text Sources
Other Literature Sources