

Use of Medicare and Department of Veterans Affairs health care by veterans with dementia: a longitudinal analysis
- PMID: 19682132
- PMCID: PMC3233990
- DOI: 10.1111/j.1532-5415.2009.02405.x
Use of Medicare and Department of Veterans Affairs health care by veterans with dementia: a longitudinal analysis
Abstract
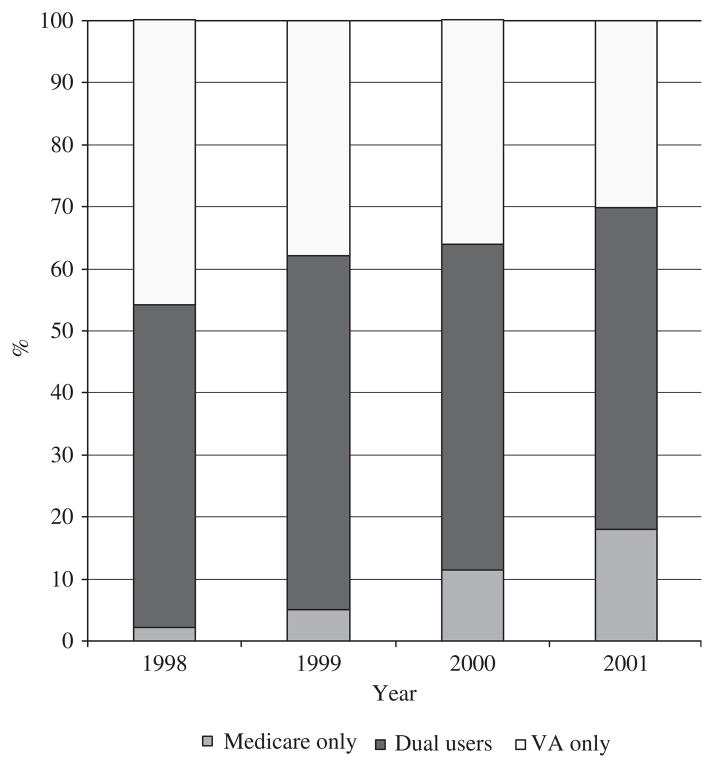
The objectives of this study were to examine longitudinal patterns of Department of Veterans Affairs (VA)-only use, dual VA and Medicare use, and Medicare-only use by veterans with dementia. Data on VA and Medicare use were obtained from VA administrative datasets and Medicare claims (1998-2001) for 2,137 male veterans who, in 1997, used some VA services, had a formal diagnosis of Alzheimer's disease or vascular dementia in the VA, and were aged 65 and older. Generalized ordered logit models were used to estimate the effects of patient characteristics on use group over time. In 1998, 41.7% of the sample were VA-only users, 55.4% were dual users, and 2.9% were Medicare-only users. By 2001, 30.4% were VA-only users, 51.5% were dual users, and 18.1% were Medicare-only users. Multivariate results show that greater likelihood of Medicare use was associated with older age, being white, being married, having higher education, having private insurance or Medicaid, having low VA priority level, and living in a nursing home or dying during the year. Higher comorbidities were associated with greater likelihood of dual use as opposed to any single system use. Alternatively, number of functional limitations was associated with greater likelihood of Medicare-only use and less likelihood of VA-only use. These results imply that different aspects of veterans' needs have differential effects on where they seek care. Efforts to coordinate care between VA and Medicare providers are necessary to ensure that patients receive high-quality care, especially patients with multiple comorbidities.
Conflict of interest statement
Figures
References
-
- Department of Veterans Affairs Strategic Plan FY2006–2011. Washington, DC: Office of the Secretary; 2006.
-
- Wright SM, Petersen LA, Lamkin RP, et al. Increasing use of Medicare services by veterans with acute myocardial infarction. Med Care. 1999;37:529–537. - PubMed
-
- Hynes DM, Stroupe KT, Greer JW, et al. Potential cost savings of erythropoietin administration in end-stage renal disease. Am J Med. 2002;112:169–175. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
