

Comèl-Netherton syndrome defined as primary immunodeficiency
- PMID: 19683336
- PMCID: PMC3685174
- DOI: 10.1016/j.jaci.2009.06.009
Comèl-Netherton syndrome defined as primary immunodeficiency
Erratum in
- J Allergy Clin Immunol. 2009 Dec;124(6):1318
Abstract
Background: Mutations in serine protease inhibitor Kazal-type 5 (SPINK5), encoding the serine protease inhibitor lympho-epithelial Kazal-type 5 related inhibitor (LEKTI), cause Comèl-Netherton syndrome, an autosomal-recessive disease characterized by congenital ichthyosis, bamboo hair, and atopic diathesis. Despite increased frequency of infections, the immunocompetence of patients with Comèl-Netherton syndrome has not been extensively investigated.
Objective: To define Comèl-Netherton syndrome as a primary immunodeficiency disorder and to explore the benefit of intravenous immunoglobulin replacement therapy.
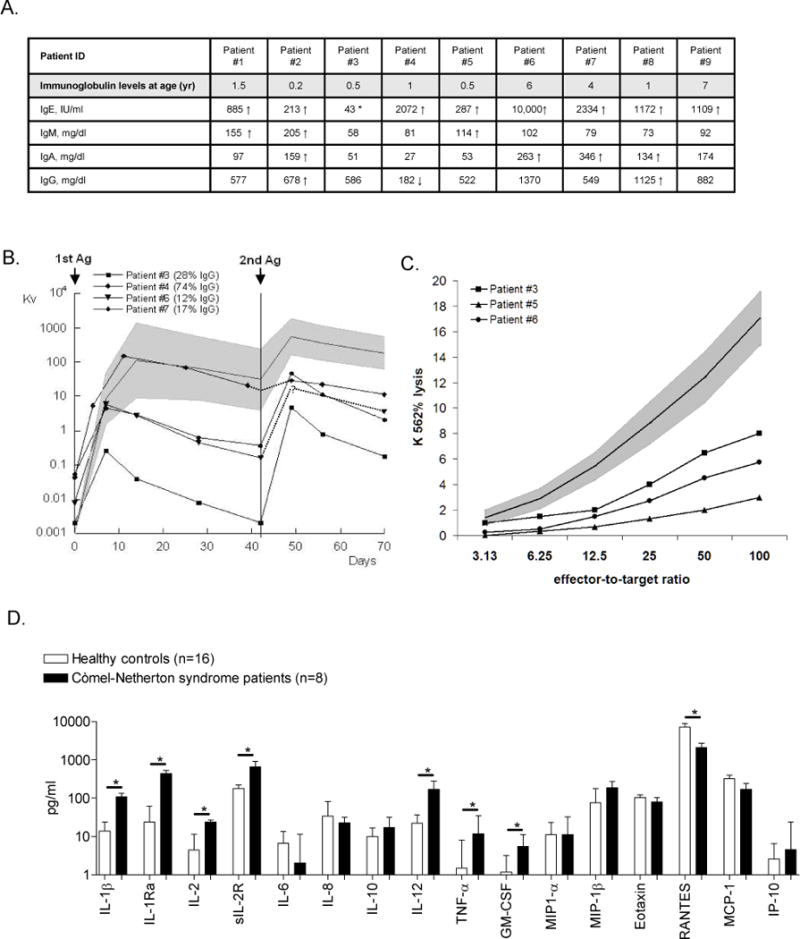
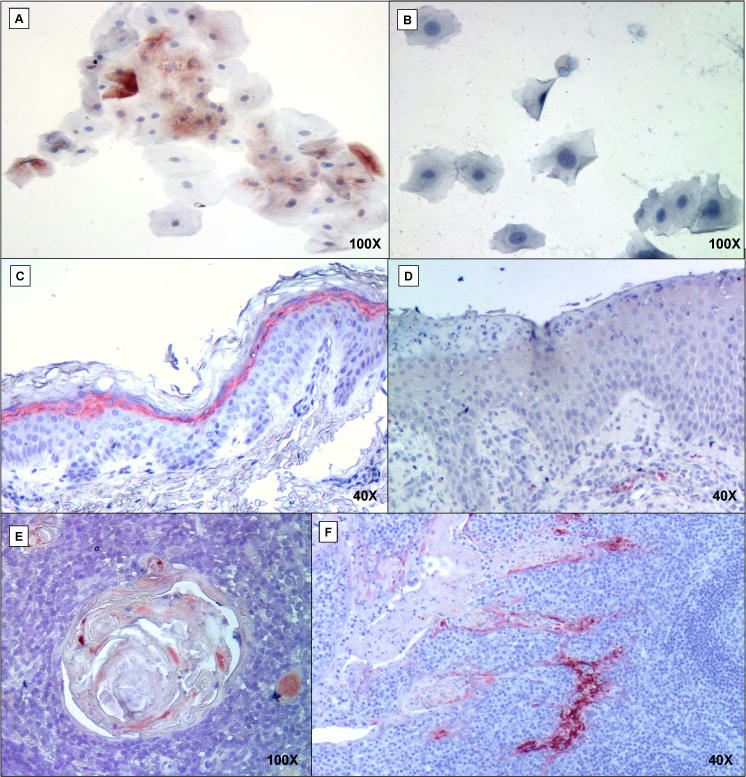
Methods: We enrolled 9 patients with Comèl-Netherton syndrome, sequenced SPINK5, and analyzed LEKTI expression by immunohistochemistry. Immune function was assessed by measuring cognate immunity, serum cytokine levels, and natural killer cell cytotoxicity.
Results: All patients presented with recurrent skin infections caused predominantly by Staphylococcus aureus. All but 1 reported recurrent respiratory tract infections; 78% had sepsis and/or pneumonia; 67% had recurrent gastrointestinal disease and failure to thrive. Mutations in SPINK5-including 6 novel mutations-were identified in 8 patients. LEKTI expression was decreased or absent in all patients. Immunologic evaluation revealed reduced memory B cells and defective responses to vaccination with Pneumovax and bacteriophage phiX174, characterized by impaired antibody amplification and class-switching. Immune dysregulation was suggested by a skewed T(h)1 phenotype and elevated proinflammatory cytokine levels, whereas serum concentrations of the chemokine (C-C motif) ligand 5 and natural killer cell cytotoxicity were decreased. Treatment with intravenous immunoglobulin resulted in remarkable clinical improvement and temporarily increased natural killer cell cytotoxicity.
Conclusion: These data provide new insights into the immunopathology of Comèl-Netherton syndrome and demonstrate that this multisystem disorder, characterized by lack of LEKTI expression in epithelial cells, is complicated by cognate and innate immunodeficiency that responds favorably to intravenous immunoglobulin therapy.
Figures

References
-
- Comel M. Ichthyosis linearis circumflexa. Dermatologica. 1949;98(3):133–6. - PubMed
-
- Netherton EW. A case for diagnosis. AMA Arch Derm Syphilol. 1951;64(1):84–5. - PubMed
-
- Wilkinson RD, Curtis GH, Hawk WA. Netherton’s Disease; Trichorrhexis Invaginata (Bamboo Hair), Congenital Ichthyosiform Erythroderma and the Atopic Diathesis. A Histopathologic Study Arch Dermatol. 1964;89:46–54. - PubMed
-
- Chavanas S, Bodemer C, Rochat A, Hamel-Teillac D, Ali M, Irvine AD, et al. Mutations in SPINK5, encoding a serine protease inhibitor, cause Netherton syndrome. Nat Genet. 2000;25(2):141–2. - PubMed
-
- Jones SK, Thomason LM, Surbrugg SK, Weston WL. Neonatal hypernatraemia in two siblings with Netherton’s syndrome. Br J Dermatol. 1986;114(6):741–3. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- AI-54843/AI/NIAID NIH HHS/United States
- R01 AI054843/AI/NIAID NIH HHS/United States
- K08 AI063267/AI/NIAID NIH HHS/United States
- R01 AI067946/AI/NIAID NIH HHS/United States
- M01 RR000037/RR/NCRR NIH HHS/United States
- AI-47040/AI/NIAID NIH HHS/United States
- R56 AI047040/AI/NIAID NIH HHS/United States
- R21 AI079731/AI/NIAID NIH HHS/United States
- AI-067946/AI/NIAID NIH HHS/United States
- AI-079731/AI/NIAID NIH HHS/United States
- R37 HD017427/HD/NICHD NIH HHS/United States
- R01 AI047040/AI/NIAID NIH HHS/United States
- R56 AI067946/AI/NIAID NIH HHS/United States
- AI-063267/AI/NIAID NIH HHS/United States
- HD-017427/HD/NICHD NIH HHS/United States
- R37 AI067946/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
