

Excluding venous thromboembolism using point of care D-dimer tests in outpatients: a diagnostic meta-analysis
- PMID: 19684102
- PMCID: PMC2727580
- DOI: 10.1136/bmj.b2990
Excluding venous thromboembolism using point of care D-dimer tests in outpatients: a diagnostic meta-analysis
Abstract
Objective: To review the evidence on the diagnostic accuracy of the currently available point of care D-dimer tests for excluding venous thromboembolism.
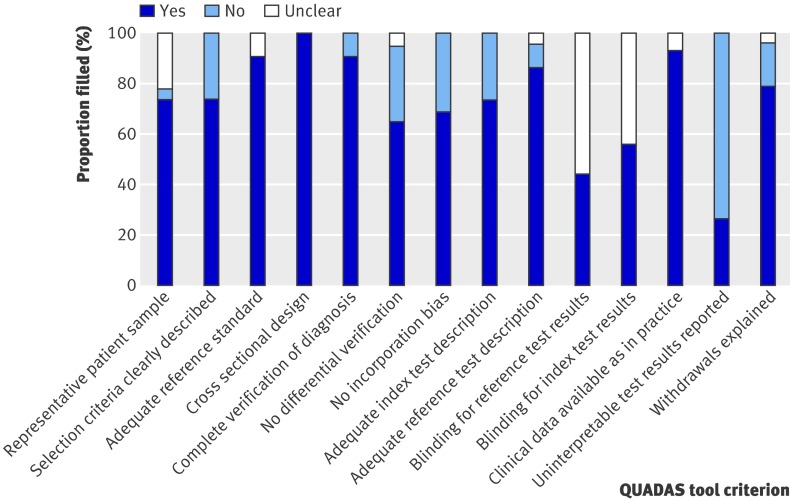
Design: Systematic review of research on the accuracy of point of care D-dimer tests, using bivariate regression to examine sources of variation and to estimate sensitivity and specificity.
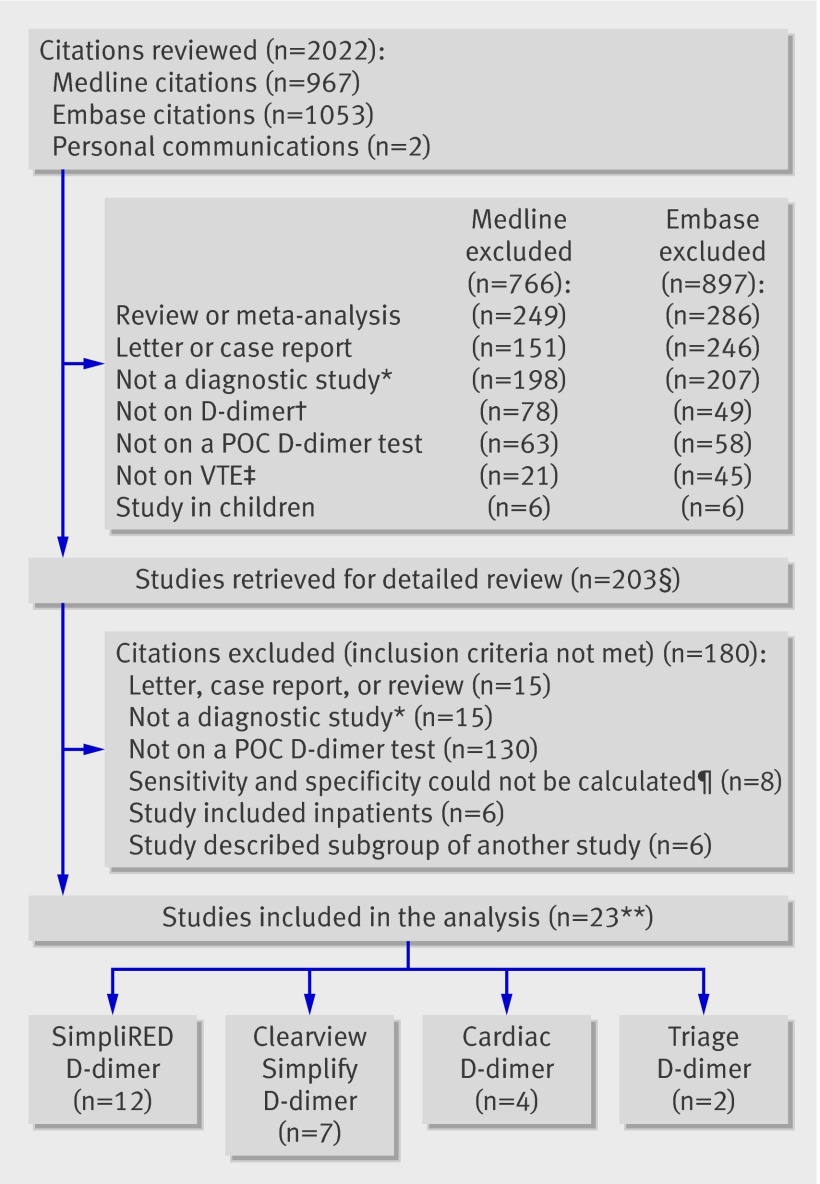
Data sources: Studies on the diagnostic accuracy of point of care D-dimer tests published between January 1995 and September 2008 and available in either Medline or Embase. Review methods The analysis included studies that compared point of care D-dimer tests with predefined reference criteria for venous thromboembolism, enrolled consecutive outpatients, and allowed for construction of a 2x2 table.
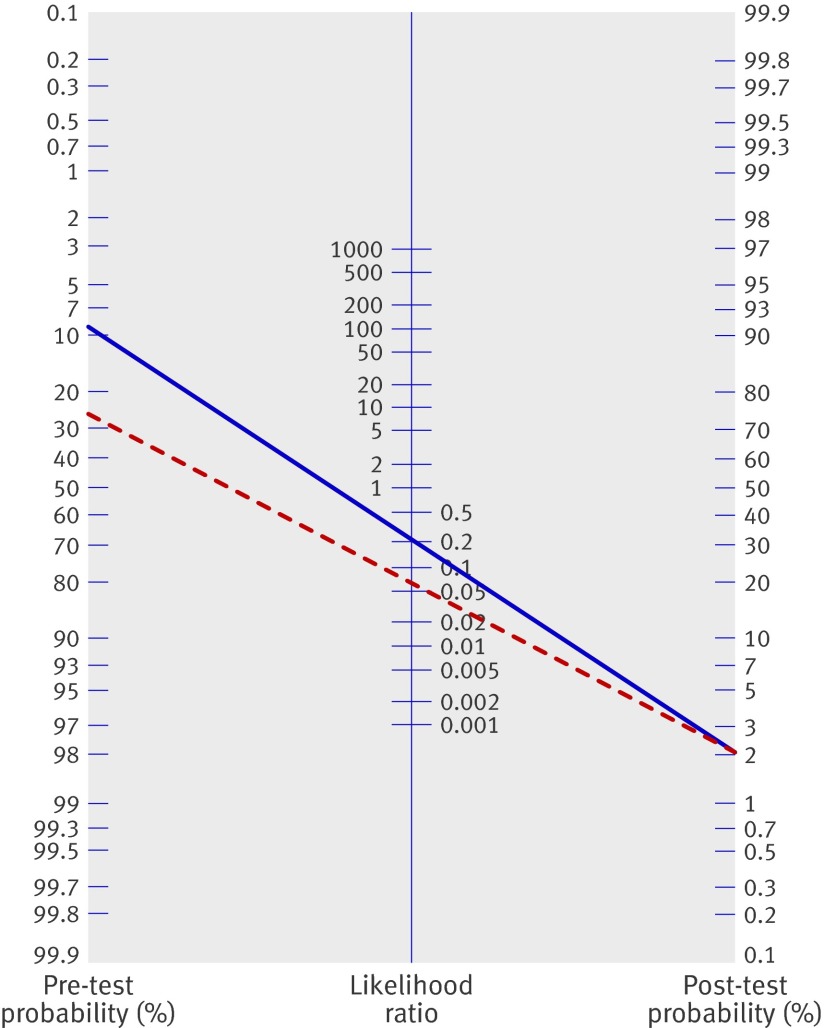
Results: 23 studies (total number of patients 13 959, range in mean age 38-65 years, range of venous thromboembolism prevalence 4-51%) were included in the meta-analysis. The studies reported two qualitative point of care D-dimer tests (SimpliRED D-dimer (n=12) and Clearview Simplify D-dimer (n=7)) and two quantitative point of care D-dimer tests (Cardiac D-dimer (n=4) and Triage D-dimer (n=2)). Overall sensitivity ranged from 0.85 (95% confidence interval 0.78 to 0.90) to 0.96 (0.91 to 0.98) and overall specificity from 0.48 (0.33 to 0.62) to 0.74 (0.69 to 0.78). The two quantitative tests Cardiac D-dimer and Triage D-dimer scored most favourably.
Conclusions: In outpatients suspected of venous thromboembolism, point of care D-dimer tests can contribute important information and guide patient management, notably in low risk patients (that is, those patients with a low score on a clinical decision rule).
Conflict of interest statement
Competing interests: The authors have conducted previous studies with point of care D-dimer tests and have received Clearview Simplify D-dimer, Cardiac D-dimer, and Triage D-dimer testkits free of charge for study purposes. Manufacturers, however, were in no way involved in the meta-analysis.
Figures

Comment in
-
Diagnosis of venous thromboembolism.BMJ. 2009 Aug 19;339:b2799. doi: 10.1136/bmj.b2799. BMJ. 2009. PMID: 19692436 No abstract available.
-
Point-of-care D-dimer tests can contribute to patient management in outpatients with suspected venous thromboembolism, particularly those at low risk.Evid Based Med. 2010 Feb;15(1):28. doi: 10.1136/ebm.15.1.28. Evid Based Med. 2010. PMID: 20176884 No abstract available.
References
-
- Oudega R, Moons KG, Hoes AW. Limited value of patient history and physical examination in diagnosing deep vein thrombosis in primary care. Fam Pract 2005;22:86-91. - PubMed
-
- Sanson BJ, Lijmer JG, Mac Gillavry MR, Turkstra F, Prins MH, Buller HR, for the ANTELOPE-Study Group. Comparison of a clinical probability estimate and two clinical models in patients with suspected pulmonary embolism. Thromb Haemost 2000;83:199-203. - PubMed
-
- Le Gal G, Righini M, Roy PM, Sanchez O, Aujesky D, Bounameaux H, et al. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann Intern Med 2006;144:165-71. - PubMed
-
- Oudega R, Moons KG, Hoes AW. Ruling out deep venous thrombosis in primary care. A simple diagnostic algorithm including D-dimer testing. Thromb Haemost 2005;94:200-5. - PubMed
-
- van Belle A, Buller HR, Huisman MV, Huisman PM, Kaasjager K, Kamphuisen PW, et al. Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA 2006;295:172-9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources