

Evaluating the cost-effectiveness of cancer patient navigation programs: conceptual and practical issues
- PMID: 19685528
- PMCID: PMC2790004
- DOI: 10.1002/cncr.24603
Evaluating the cost-effectiveness of cancer patient navigation programs: conceptual and practical issues
Abstract
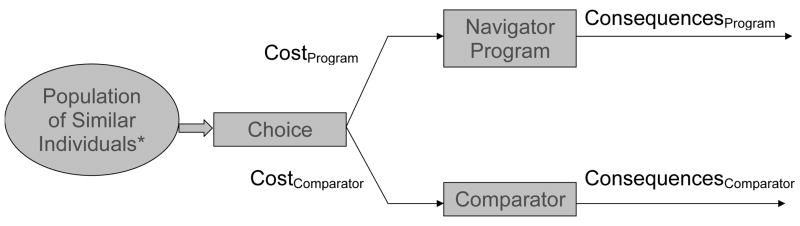
Patient navigators-individuals who assist patients through the healthcare system to improve access to and understanding of their health and healthcare-are increasingly used for underserved individuals at risk for or with cancer. Navigation programs can improve access, but it is unclear whether they improve the efficiency and efficacy of cancer diagnostic and therapeutic services at a reasonable cost, such that they would be considered cost-effective. In the current study, the authors outline a conceptual model for evaluating the cost-effectiveness of cancer navigation programs. They describe how this model is being applied to the Patient Navigation Research Program, a multicenter study supported by the National Cancer Institute's Center to Reduce Cancer Health Disparities. The Patient Navigation Research Program is testing navigation interventions that aim to reduce time to delivery of quality cancer care (noncancer resolution or cancer diagnosis and treatment) after identification of a screening abnormality. Examples of challenges to evaluating cost-effectiveness of navigation programs include the heterogeneity of navigation programs, the sometimes distant relation between navigation programs and outcome of interest (eg, improving access to prompt diagnostic resolution and life-years gained), and accounting for factors in underserved populations that may influence both access to services and outcomes. In this article, the authors discuss several strategies for addressing these barriers. Evaluating the costs and impact of navigation will require some novel methods, but will be critical in recommendations concerning dissemination of navigation programs.
(c) 2009 American Cancer Society.
Figures
References
-
- Strzelczyk JJ, Dignan MB. Disparities in adherence to recommended followup on screening mammography: interaction of sociodemographic factors. Ethn Dis. 2002;12(1):77–86. - PubMed
-
- Gwyn K, Bondy ML, Cohen DS, et al. Racial differences in diagnosis, treatment, and clinical delays in a population-based study of patients with newly diagnosed breast carcinoma. Cancer. 2004;100(8):1595–604. - PubMed
-
- Center to Reduce Cancer Health Disparities. National Cancer Institute, National Institute of Health Publication No. 07–6131. 2007. Economic costs of cancer health disparities.
-
- Lurie JD, Welch HG. Diagnostic testing following fecal occult blood screening in the elderly. J Natl Cancer Inst. 1999;91(19):1641–6. - PubMed
-
- Baig N, Myers RE, Turner BJ, et al. Physician-reported reasons for limited follow-up of patients with a positive fecal occult blood test screening result. Am J Gastroenterol. 2003;98(9):2078–81. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 CA116875/CA/NCI NIH HHS/United States
- U01 CA116924/CA/NCI NIH HHS/United States
- U01 CA88283/CA/NCI NIH HHS/United States
- U01 CA116892/CA/NCI NIH HHS/United States
- U01 CA116937/CA/NCI NIH HHS/United States
- N261200700048U/PHS HHS/United States
- HHSN261200700048U/CA/NCI NIH HHS/United States
- UL1 RR025755/RR/NCRR NIH HHS/United States
- U01 CA116925/CA/NCI NIH HHS/United States
- 263-FQ-612391/PHS HHS/United States
- U01 CA117281/CA/NCI NIH HHS/United States
- U01 CA116885/CA/NCI NIH HHS/United States
- U01 CA116903/CA/NCI NIH HHS/United States
- U01 CA088283/CA/NCI NIH HHS/United States
- KO5 CA96940/CA/NCI NIH HHS/United States
- K05 CA096940/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
