

An 8-year longitudinal study of the natural history of threshold, subthreshold, and partial eating disorders from a community sample of adolescents
- PMID: 19685955
- PMCID: PMC2849679
- DOI: 10.1037/a0016481
An 8-year longitudinal study of the natural history of threshold, subthreshold, and partial eating disorders from a community sample of adolescents
Abstract
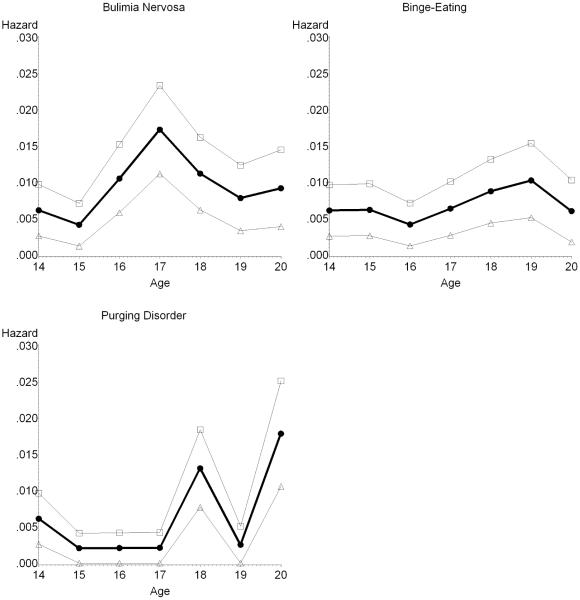
The authors examined the natural history of threshold, subthreshold, and partial eating disorders in a community sample of 496 adolescent girls who completed annual diagnostic interviews over an 8-year period. Lifetime prevalence by age 20 years was 0.6% and 0.6% for threshold and subthreshold anorexia nervosa (AN), 1.6% and 6.1% for threshold and subthreshold bulimia nervosa (BN), 1.0% and 4.6% for threshold and subthreshold binge-eating disorder (BED), and 4.4% for purging disorder (PD). Overall, 12% of adolescents experienced some form of eating disorder. Subthreshold BN and BED and threshold PD were associated with elevated treatment, impairment, and distress. Peak age of onset was 17-18 years for BN and BED and 18-20 years for PD. Average episode duration in months was 3.9 for BN and BED and 5.1 for PD. One-year recovery rates ranged from 91% to 96%. Relapse rates were 41% for BN, 33% for BED, and 5% for PD. For BN and BED, subthreshold cases often progressed to threshold cases and diagnostic crossover was most likely for these disorders. Results suggest that subthreshold eating disorders are more prevalent than threshold eating disorders and are associated with marked impairment.
Figures
References
-
- Agras WS, Walsh BT, Fairburn CG, Wilson GT, Kraemer HC. A multicenter comparison of cognitive-behavioral therapy and interpersonal therapy for bulimia nervosa. Archives of General Psychiatry. 2000;57:459–466. - PubMed
-
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 4th ed. Author; Washington, DC: 1994.
-
- Buss AH, Plomin R. Temperament: Early developing personality traits. Lawrence Erlbaum; Hillsdale, NJ: 1984.
-
- Cachelin FM, Striegel-Moore RH, Elder KA, Pike KM, Wilfley DE, Fairburn CG. Natural course of a community sample of women with binge eating disorder. International Journal of Eating Disorders. 1999;25:45–54. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
