

Magnetic resonance imaging in sclerotic-type chronic graft-vs-host disease
- PMID: 19687424
- PMCID: PMC8375560
- DOI: 10.1001/archdermatol.2009.78
Magnetic resonance imaging in sclerotic-type chronic graft-vs-host disease
Abstract
Background: Sclerotic-type chronic graft-vs-host disease (cGVHD) of the skin is an uncommon but potentially debilitating sequela of allogeneic hematopoietic stem cell transplantation. There is no standardized assessment measure for this form of cGVHD. Because a full-thickness incisional biopsy specimen to the level of the fascia may be needed to make a definitive histologic diagnosis of cGVHD-related fasciitis, a noninvasive technique for the assessment and monitoring of sclerotic-type cGVHD, particularly cGVHD-related fasciitis, would be of potential value.
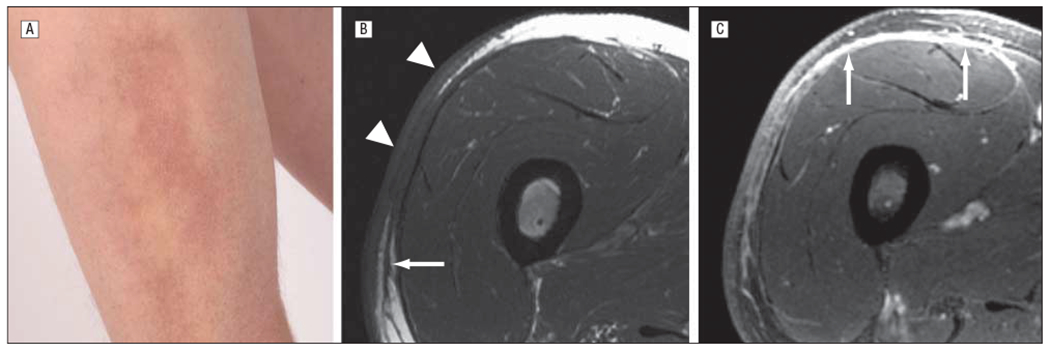
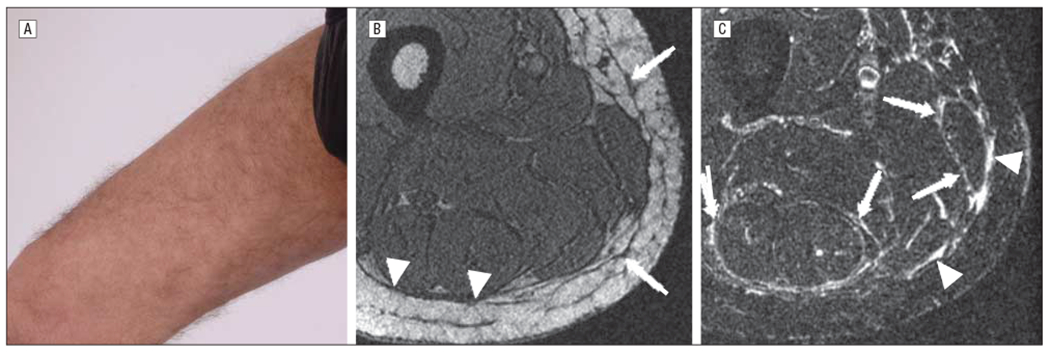
Observations: Sixty-two consecutive patients with cGVHD following allogeneic hematopoietic stem cell transplantation were evaluated for sclerotic skin disease. Forty-four patients (71%) had cutaneous cGVHD, and 28 patients (45%) had evidence of sclerotic involvement based on physical examination findings. Fifteen patients agreed to undergo research magnetic resonance imaging to evaluate quantifiable changes in the dermis, subcutaneous tissue, and muscle. Among 15 patients, magnetic resonance imaging identified abnormalities in the skin in 7 (47%), subcutaneous fibrous septa in 13 (87%), deep fascia in 12 (80%), epimysium in 9 (60%), and muscle in 3 (20%).
Conclusions: Magnetic resonance imaging should be considered in the evaluation of patients with cGVHD suspected of having subcutaneous or fascial involvement. Additional studies are needed to validate this noninvasive modality for serial monitoring of disease activity and response to therapy. Trial Registration clinicaltrials.gov Identifier: NCT00331968.
Figures
References
-
- Filipovich AH, Weisdorf D, Pavletic S, et al.National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease, I: Diagnosis and Staging Working Group report. Biol Blood Marrow Transplant. 2005;11(12):945–956. - PubMed
-
- Hymes SR, Turner ML, Champlin RE, Couriel DR. Cutaneous manifestations of chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2006;12(11):1101–1113. - PubMed
-
- Schaffer JV, McNiff JM, Seropian S, Cooper DL, Bolognia JL. Lichen sclerosus and eosinophilic fasciitis as manifestations of chronic graft-versus-host disease: expanding the sclerodermoid spectrum. J Am Acad Dermatol. 2005;53(4):591–601. - PubMed
-
- Häusermann P, Walter RB, Halter J, et al.Cutaneous graft-versus-host disease: a guide for the dermatologist. Dermatology. 2008;216(4):287–304. - PubMed
-
- Kimball AB, Summers RM, Turner M, et al.Magnetic resonance imaging detection of occult skin and subcutaneous abnormalities in juvenile dermatomyositis: implications for diagnosis and therapy. Arthritis Rheum. 2000;43(8):1866–1873. - PubMed
