

Sleep-disordered breathing and mortality: a prospective cohort study
- PMID: 19688045
- PMCID: PMC2722083
- DOI: 10.1371/journal.pmed.1000132
Sleep-disordered breathing and mortality: a prospective cohort study
Abstract
Background: Sleep-disordered breathing is a common condition associated with adverse health outcomes including hypertension and cardiovascular disease. The overall objective of this study was to determine whether sleep-disordered breathing and its sequelae of intermittent hypoxemia and recurrent arousals are associated with mortality in a community sample of adults aged 40 years or older.
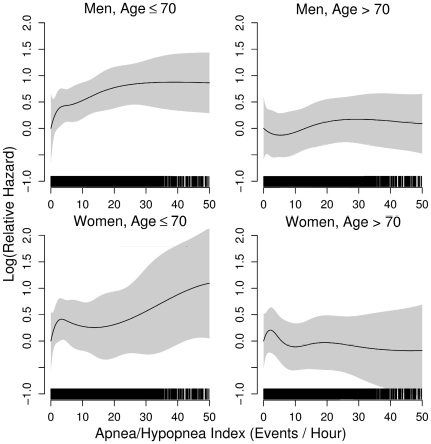
Methods and findings: We prospectively examined whether sleep-disordered breathing was associated with an increased risk of death from any cause in 6,441 men and women participating in the Sleep Heart Health Study. Sleep-disordered breathing was assessed with the apnea-hypopnea index (AHI) based on an in-home polysomnogram. Survival analysis and proportional hazards regression models were used to calculate hazard ratios for mortality after adjusting for age, sex, race, smoking status, body mass index, and prevalent medical conditions. The average follow-up period for the cohort was 8.2 y during which 1,047 participants (587 men and 460 women) died. Compared to those without sleep-disordered breathing (AHI: <5 events/h), the fully adjusted hazard ratios for all-cause mortality in those with mild (AHI: 5.0-14.9 events/h), moderate (AHI: 15.0-29.9 events/h), and severe (AHI: >or=30.0 events/h) sleep-disordered breathing were 0.93 (95% CI: 0.80-1.08), 1.17 (95% CI: 0.97-1.42), and 1.46 (95% CI: 1.14-1.86), respectively. Stratified analyses by sex and age showed that the increased risk of death associated with severe sleep-disordered breathing was statistically significant in men aged 40-70 y (hazard ratio: 2.09; 95% CI: 1.31-3.33). Measures of sleep-related intermittent hypoxemia, but not sleep fragmentation, were independently associated with all-cause mortality. Coronary artery disease-related mortality associated with sleep-disordered breathing showed a pattern of association similar to all-cause mortality.
Conclusions: Sleep-disordered breathing is associated with all-cause mortality and specifically that due to coronary artery disease, particularly in men aged 40-70 y with severe sleep-disordered breathing. Please see later in the article for the Editors' Summary.
Conflict of interest statement
NMP received honoraria and travel support for continuing medical education lectures or symposia sponsored by Respironics and Resmed Inc. DMR is currently the holder (through New York University) of multiple patents licensed to Covidian and Fisher & Paykel Healthcare on the use of nasal CPAP, the primary treatment of obstructive sleep apnea, and to Advance Brain Monitoring, Protech on diagnostic tools for use in ambulatory monitoring of sleep apnea, and recieves royalties from these. DMR has also held industry-sponsored grants relating to sleep and sleep-disordered breathing treatments with Restore Medical, St. Jude Medical, Guidant (Boston Scientific), Protech, Advanced Brain Monitoring, and Korosensor. At no time were any of the activities of DMR in the Sleep Heart Health Study data collection or analysis directly related to any of his listed activities in ways that compromised the study, as reviewed annually by the Steering Committee. SR has National Institutes of Health grants that fund research into the association of sleep disorders and health outcomes. SR is a member of the Sleep Research Society Board of Directors. SR is the Principal Investigator for a contract between University Hospitals of Cleveland and Dymedix, Inc. to validate sleep signals of sleep apnea diagnosis. MLU has a Baxter Healthcare Grant (Reanalysis of the HEMO Study using novel analytic approaches). MLU is personally unaware of a Baxter sleep product and this support did not influence his contribution to this work.
Figures

Comment in
-
Sleep-disordered breathing and all-cause mortality in the sleep heart health study. Commentary.Postgrad Med. 2009 Nov;121(6):197-9. doi: 10.3810/pgm.2009.11.2088. Postgrad Med. 2009. PMID: 19940430 No abstract available.
References
-
- Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165:1217–1239. - PubMed
-
- He J, Kryger MH, Zorick FJ, Conway W, Roth T. Mortality and apnea index in obstructive sleep apnea. Experience in 385 male patients. Chest. 1988;94:9–14. - PubMed
-
- Gonzalez-Rothi RJ, Foresman GE, Block AJ. Do patients with sleep apnea die in their sleep? Chest. 1988;94:531–538. - PubMed
Publication types
MeSH terms
Grants and funding
- U01-HL53937/HL/NHLBI NIH HHS/United States
- U01 HL053916/HL/NHLBI NIH HHS/United States
- U01-HL53940/HL/NHLBI NIH HHS/United States
- U01-HL53934/HL/NHLBI NIH HHS/United States
- U01-HL53931/HL/NHLBI NIH HHS/United States
- U01-HL63429/HL/NHLBI NIH HHS/United States
- U01-HL53916/HL/NHLBI NIH HHS/United States
- U01-HL53941/HL/NHLBI NIH HHS/United States
- U01 HL053941/HL/NHLBI NIH HHS/United States
- U01 HL053937/HL/NHLBI NIH HHS/United States
- K25 EB003491/EB/NIBIB NIH HHS/United States
- U01 HL053931/HL/NHLBI NIH HHS/United States
- U01-HL63463/HL/NHLBI NIH HHS/United States
- U01 HL063463/HL/NHLBI NIH HHS/United States
- U01-HL53938/HL/NHLBI NIH HHS/United States
- U01 HL053938/HL/NHLBI NIH HHS/United States
- U01 HL053934/HL/NHLBI NIH HHS/United States
- U01 HL063429/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
