Cancer of unknown primary finally revealed to be a metastatic prostate cancer: a case report
- PMID: 19688071
- PMCID: PMC2699091
- DOI: 10.4143/crt.2009.41.1.45
Cancer of unknown primary finally revealed to be a metastatic prostate cancer: a case report
Abstract
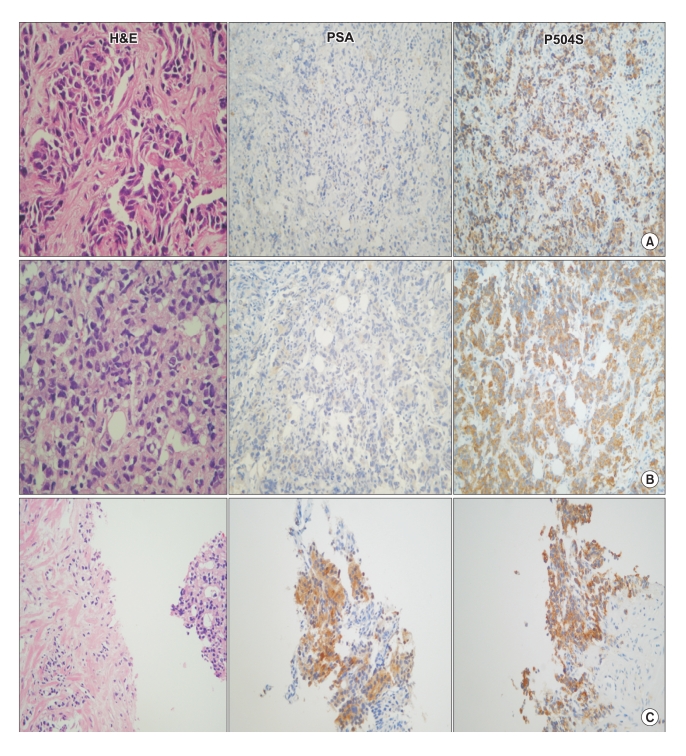
The vast majority of patients with metastatic prostate cancer present with bone metastases and high prostate specific antigen (PSA) level. Rarely, prostate cancer can develop in patients with normal PSA level. Here, we report a patient who presented with a periureteral tumor of unknown primary site that was confirmed as prostate adenocarcinoma after three years with using specific immunohistochemical examination. A 64-year old man was admitted to our hospital with left flank pain associated with masses on the left pelvic cavity with left hydronephrosis. All tumor markers including CEA, CA19-9, and PSA were within the normal range. After an exploratory mass excision and left nephrectomy, the pelvic mass was diagnosed as poorly differentiated carcinoma without specific positive immunohistochemical markers. At that time, we treated him as having a cancer of unknown primary site. After approximately three years later, he revisited the hospital with a complaint of right shoulder pain. A right scapular mass was newly detected with a high serum PSA level (101.7 ng/ml). Tissues from the scapular mass and prostate revealed prostate cancer with positive immunoreactivity for P504S, a new prostate cancer-specific gene. The histological findings were the same as the previous pelvic mass; however, positive staining for PSA was observed only in the prostate mass. This case demonstrates a patient with prostate cancer and negative serological test and tissue staining that turned out to be positive during progression. We suggest the usefulness of newly developed immunohistochemical markers such as P504S to determine the specific primary site of metastatic poorly differentiated adenocarcinoma in men.
Keywords: Cancer of unknown primary; Metastatic prostate cancer; P504S.
Figures


References
-
- Pavlidis N, Briasoulis E, Hainsworth J, Greco FA. Diagnostic and therapeutic management of cancer of an unknown primary. Eur J Cancer. 2003;39:1990–2005. - PubMed
-
- Ministry of health and welfare; Central cancer registry center; regional cancer registry. Annual report of the cause of death in Korea 2006.
-
- Varadhachary GR, Abbruzzese JL, Lenzi R. Diagnostic strategies for unknown primary cancer. Cancer. 2004;100:1776–1785. - PubMed
-
- Greco FA, Hainsworth JD. Cancer of unknown primary site. In: DeVita VT Jr, Hellman S, Rosenberg SA, editors. Cancer: principles and practice of oncology. 7th ed. Philadelphia, PA: Lippincott; 2005. pp. 2213–2236.
-
- Polascik TJ, Oesterling JE, Partin AW. Prostate specific antigen: a decade of discovery: what we have learned and where we are going. J Urol. 1999;162:293–306. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous