

Phonation threshold pressure estimation using electroglottography in an airflow redirection system
- PMID: 19688842
- PMCID: PMC2789983
- DOI: 10.1002/lary.20611
Phonation threshold pressure estimation using electroglottography in an airflow redirection system
Abstract
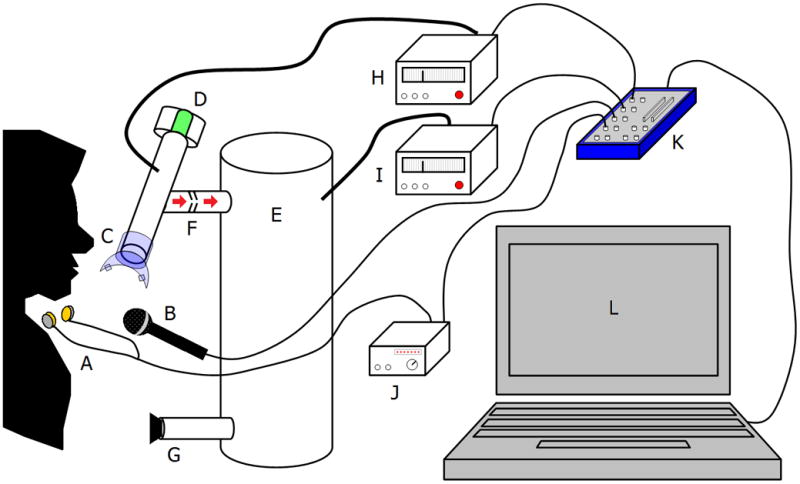
Objectives/hypothesis: The present study proposed to estimate phonation threshold pressure (PTP) noninvasively using airflow redirection into a pneumatic capacitance system.
Study design: Prospective study.
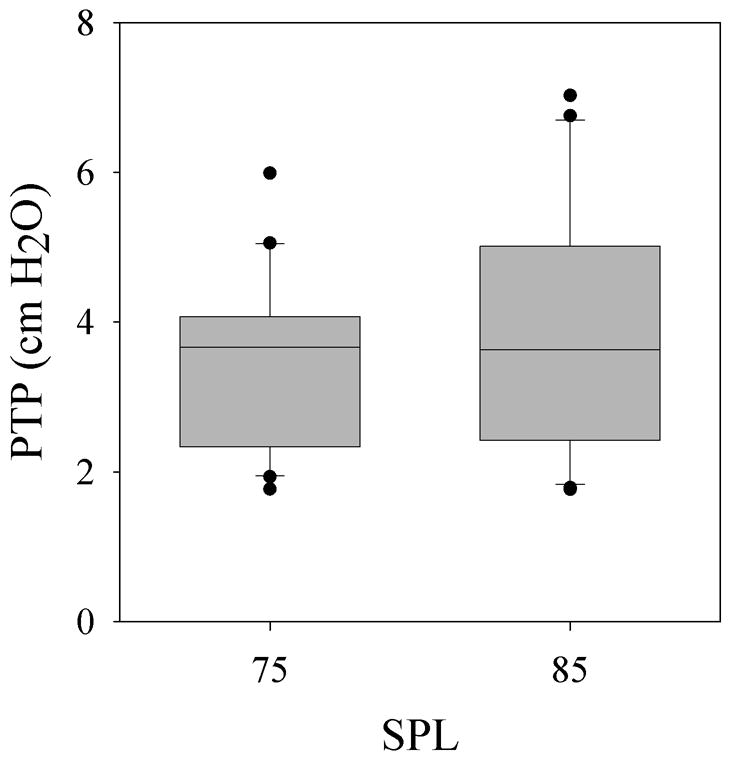
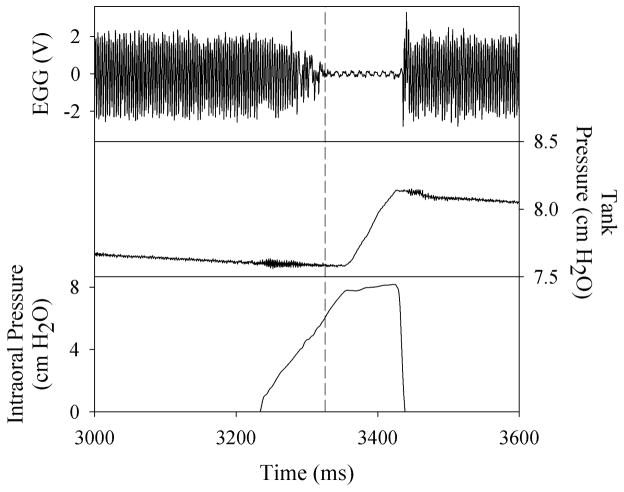
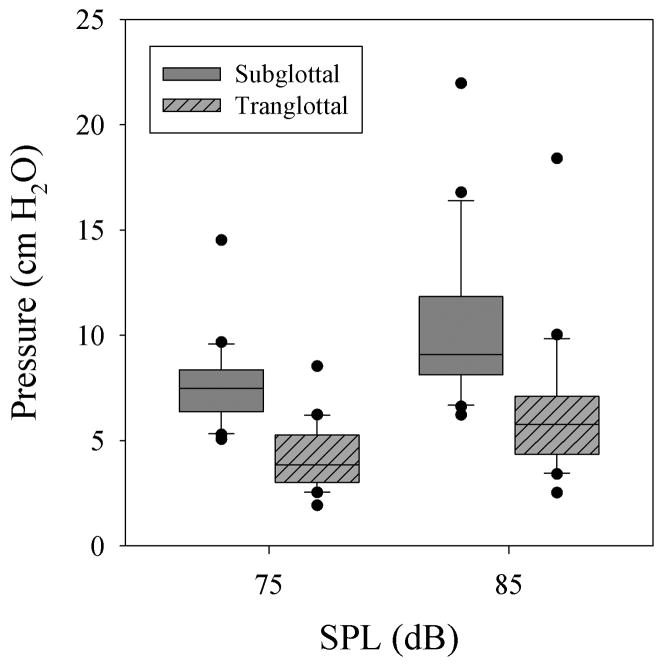
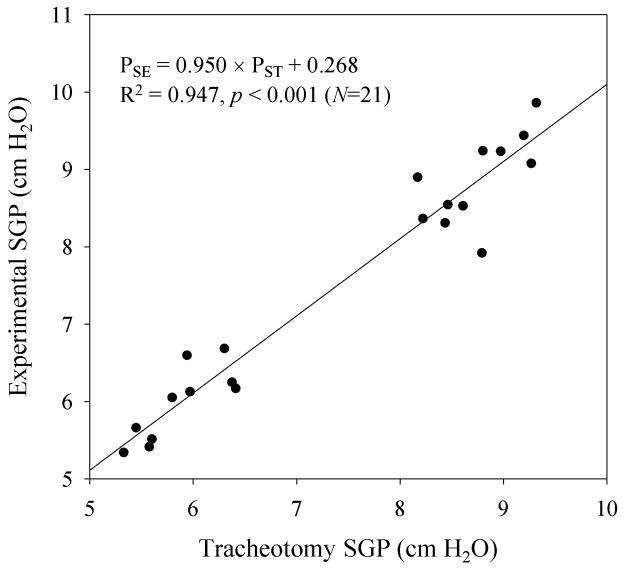
Methods: Subjects phonated into the device, which interrupts airflow mechanically and redirects the flow into a pneumatic capacitor. Five interruptions were effected per trial. PTP was estimated as the difference between subglottal pressure (SGP) and transglottal pressure at phonation offset. The novel method was tested for consistency in 20 normal human subjects at low (75 dB) and high (85 dB) sound pressure levels. The device was tested for validity on a tracheotomy patient.
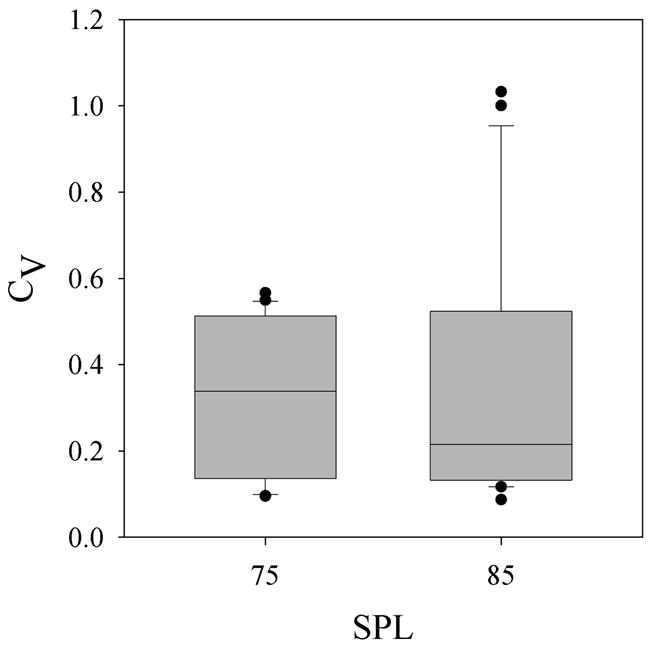
Results: Mean SGP was 9.02 +/- 3.27 cm H(2)O, and mean PTP was 3.68 +/- 1.41 cm H(2)O. Intrasubject coefficient of variation, a measure of intrasubject consistency, was 0.33 +/- 0.23. Statistically significant differences existed between the means of SGP but not PTP at 75 dB and 85 dB. The correlation coefficient between accepted and experimental SGP in a tracheotomy patient was 0.947 (P < .001).
Conclusions: Measurements corresponded well to previously reported values, and intrasubject variability was low, indicating the device was consistent. Testing on a tracheotomy patient demonstrated validity. More research is needed to determine the sensitivity and specificity of the device in differentiating between normal and pathological voices. This device may have clinical application as a noninvasive and reliable method of estimating PTP and indicating that laryngeal health is likely abnormal.
Figures
References
-
- Titze IR. The physics of small-amplitude oscillation of the vocal folds. J Acoust Soc Am. 1988;83:1536–1552. - PubMed
-
- Titze IR, Schmidt SS, Titze MR. Phonation threshold pressure in a physical model of the vocal fold mucosa. J Acoust Soc Am. 1995;97:3080–3084. - PubMed
-
- Jiang J, O’Mara T, Chen HJ, Stern JI, Vlagos D, Hanson D. Aerodynamic measurements of patients with Parkinson’s disease. J Voice. 1999;13:583–591. - PubMed
-
- Hirano S, Bless DM, Rousseau B, et al. Prevention of vocal fold scarring by topical injection of hepatocyte growth factor in a rabbit model. Laryngoscope. 2004;114:548–556. - PubMed
-
- Rousseau B, Tateya I, Lim X, Munoz-del-Rio A, Bless DM. Investigation of anti-hyaluronidase treatment on vocal fold wound healing. J Voice. 2006;20:443–451. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
