

The added value of longitudinal black-blood cardiovascular magnetic resonance angiography in the cross sectional identification of carotid atherosclerotic ulceration
- PMID: 19689816
- PMCID: PMC2737539
- DOI: 10.1186/1532-429X-11-31
The added value of longitudinal black-blood cardiovascular magnetic resonance angiography in the cross sectional identification of carotid atherosclerotic ulceration
Abstract
Background: Carotid atherosclerotic ulceration is a significant source of stroke. This study evaluates the efficacy of adding longitudinal black-blood (BB) cardiovascular magnetic resonance (CMR) angiography to cross-sectional CMR images in the identification of carotid atherosclerotic ulceration.
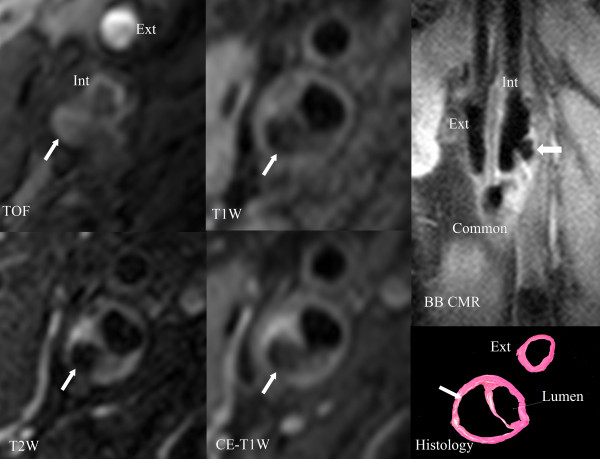
Methods: Thirty-two subjects (30 males and two females with ages between 48 and 83 years) scheduled for carotid endarterectomy were imaged on a 1.5T GE Signa scanner using multisequence [3D time-of-flight, T1, proton density, T2, contrast enhanced T1], cross-sectional CMR images and longitudinal BB CMR angiography (0.625 x 0.625 mm/pixel). Two rounds of review (round 1: cross-sectional CMR images alone and round 2: cross-sectional CMR images plus longitudinal BB CMR angiography) were conducted for the presence and volume measurements of ulceration. Ulceration was defined as a distinct depression into the plaque containing blood flow signal on cross-sectional CMR and longitudinal BB CMR angiography.
Results: Of the 32 plaques examined by histology, 17 contained 21 ulcers. Using the longitudinal BB CMR angiography sequence in addition to the cross-sectional CMR images in round 2, the sensitivity improved to 80% for ulcers of at least 6 mm3 in volume by histology and 52.4% for all ulcers, compared to 30% and 23.8% in round 1, respectively. There was a slight decline in specificity from 88.2% to 82.3%, though both the positive and negative predictive values increased modestly from 71.4% to 78.6% and from 48.4% to 58.3%, respectively.
Conclusion: The addition of longitudinal BB CMR angiography to multisequence cross-sectional CMR images increases accuracy in the identification of carotid atherosclerotic ulceration.
Figures





References
-
- Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, Hailpern SM, Ho M, Howard V, Kissela B, Kittner S, Lloyd-Jones D, McDermott M, Meigs J, Moy C, Nichol G, O'Donnell C, Roger V, Sorlie P, Steinberger J, Thom T, Wilson M, Hong Y. Heart disease and stroke statistics 2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25–e146. doi: 10.1161/CIRCULATIONAHA.107.187998. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
