

Chlorproguanil-dapsone-artesunate versus artemether-lumefantrine: a randomized, double-blind phase III trial in African children and adolescents with uncomplicated Plasmodium falciparum malaria
- PMID: 19690618
- PMCID: PMC2724683
- DOI: 10.1371/journal.pone.0006682
Chlorproguanil-dapsone-artesunate versus artemether-lumefantrine: a randomized, double-blind phase III trial in African children and adolescents with uncomplicated Plasmodium falciparum malaria
Abstract
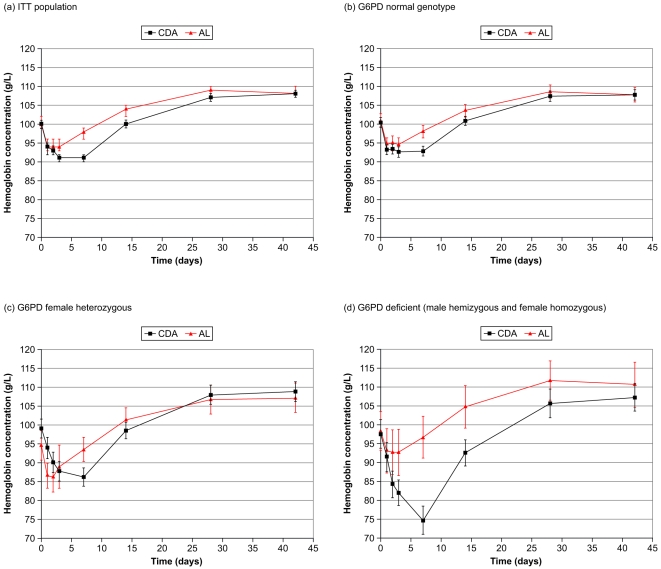
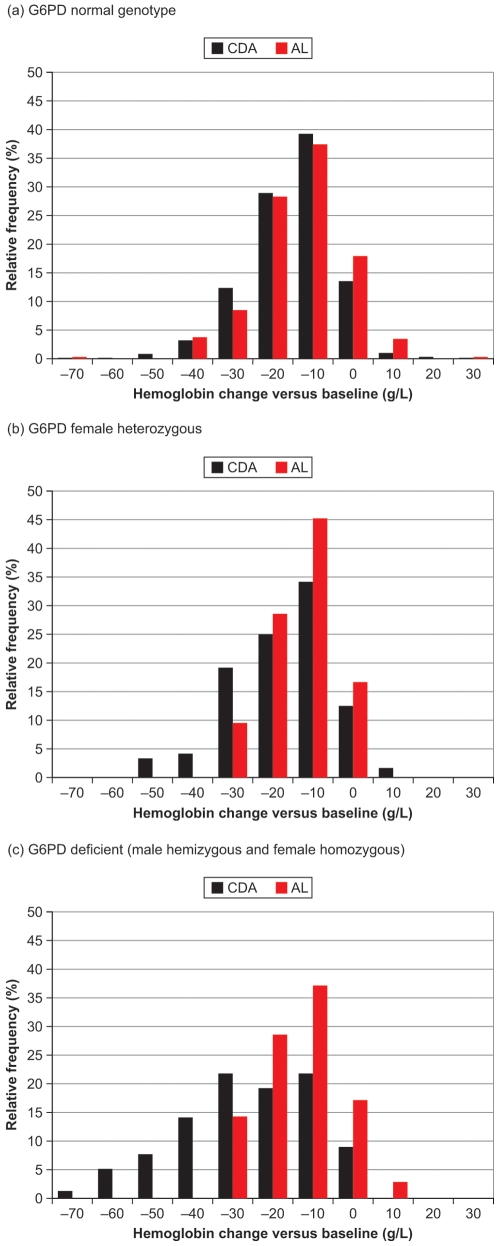
Background: Chlorproguanil-dapsone-artesunate (CDA) was developed as an affordable, simple, fixed-dose artemisinin-based combination therapy for use in Africa. This trial was a randomized parallel-group, double-blind, double-dummy study to compare CDA and artemether-lumefantrine (AL) efficacy in uncomplicated Plasmodium falciparum malaria and further define the CDA safety profile, particularly its hematological safety in glucose-6-phosphate dehydrogenase (G6PD) -deficient patients.
Methods and findings: The trial was conducted at medical centers at 11 sites in five African countries between June 2006 and August 2007. 1372 patients (> or =1 to <15 years old, median age 3 years) with acute uncomplicated P. falciparum malaria were randomized (2:1) to receive CDA 2/2.5/4 mg/kg once daily for three days (N = 914) or six-doses of AL over three days (N = 458). Non-inferiority of CDA versus AL for efficacy was evaluated in the Day 28 per-protocol (PP) population using parasitological cure (polymerase chain reaction [PCR]-corrected). Cure rates were 94.1% (703/747) for CDA and 97.4% (369/379) for AL (treatment difference -3.3%, 95%CI -5.6, -0.9). CDA was non-inferior to AL, but there was simultaneous superiority of AL (upper 95%CI limit <0). Adequate clinical and parasitological response at Day 28 (uncorrected for reinfection) was 79% (604/765) with CDA and 83% (315/381) with AL. In patients with a G6PD-deficient genotype (94/603 [16%] hemizygous males, 22/598 [4%] homozygous females), CDA had the propensity to cause severe and clinically concerning hemoglobin decreases: the mean hemoglobin nadir was 75 g/L (95%CI 71, 79) at Day 7 versus 97 g/L (95%CI 91, 102) for AL. There were three deaths, unrelated to study medication (two with CDA, one with AL).
Conclusions: Although parasitologically effective at Day 28, the hemolytic potential of CDA in G6PD-deficient patients makes it unsuitable for use in a public health setting in Africa.
Trial registration: ClinicalTrials.Gov NCT00344006.
Conflict of interest statement
Figures

References
-
- World Health Organisation. World Malaria Report. Geneva: World Health Organisation; 2005. Available online at: http://rbm.who.int/wmr2005/ (Last accessed 23rd August, 2008)
-
- Bousema JT, Schneider P, Gouagna LC, Drakeley CJ, Tostmann A, et al. Moderate effect of artemisinin-based combination therapy on transmission of Plasmodium falciparum. J Infect Dis. 2006;193:1151–1159. - PubMed
-
- World Health Organisation. Guidelines for the treatment of malaria. Geneva: World Health Organisation; 2006. Available online at: http://malaria.who.int/docs/TreatmentGuidelines2006.pdf (Last accessed 22nd August, 2008)
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
