

Epidemiology of Obstructive Sleep Apnea: a Population-based Perspective
- PMID: 19690624
- PMCID: PMC2727690
- DOI: 10.1586/17476348.2.3.349
Epidemiology of Obstructive Sleep Apnea: a Population-based Perspective
Abstract
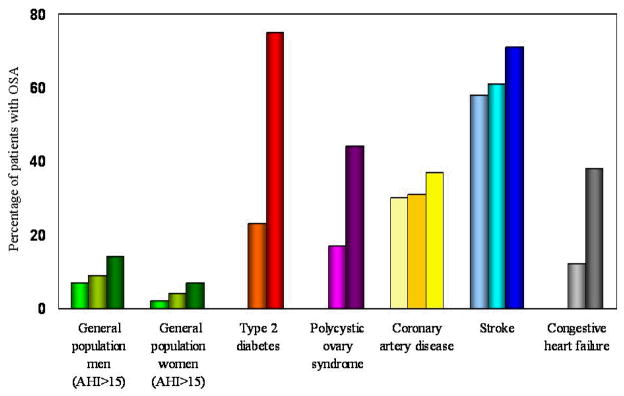
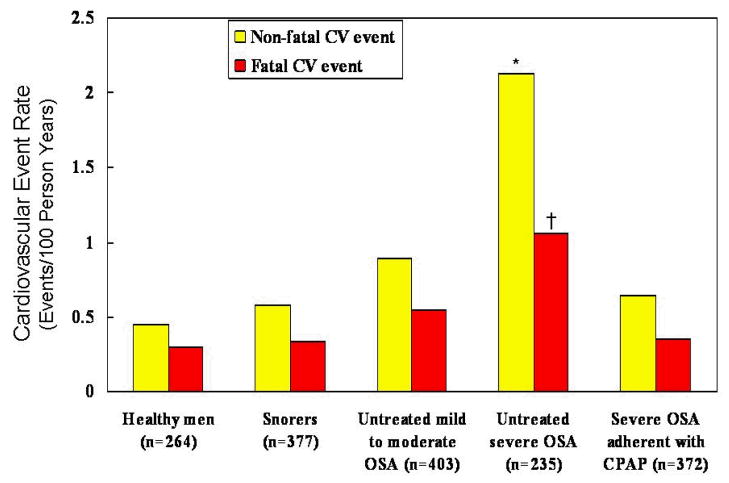
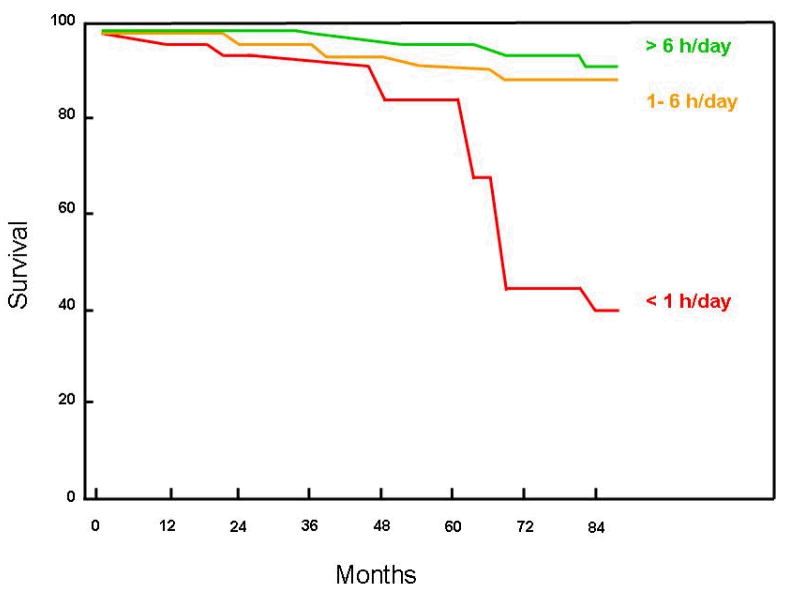
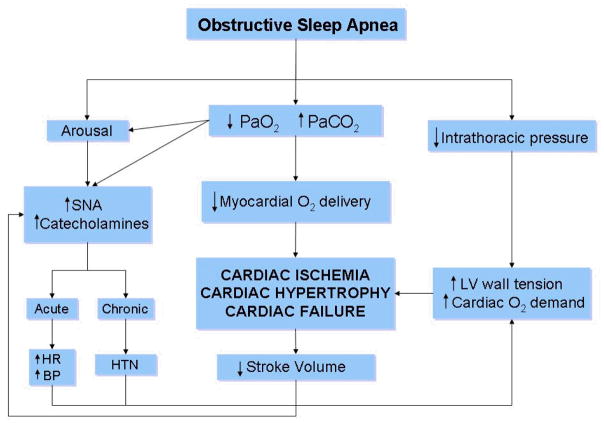
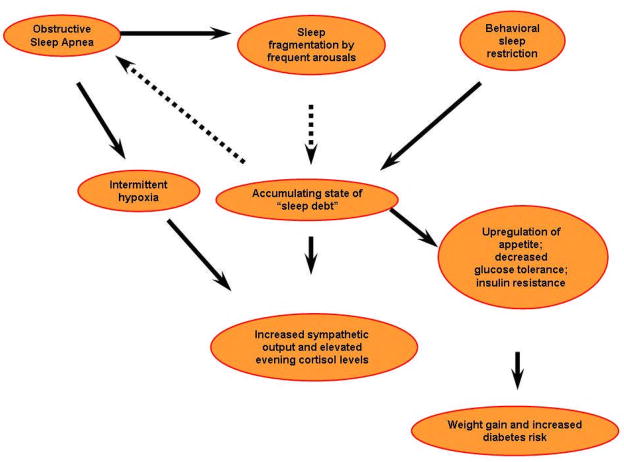
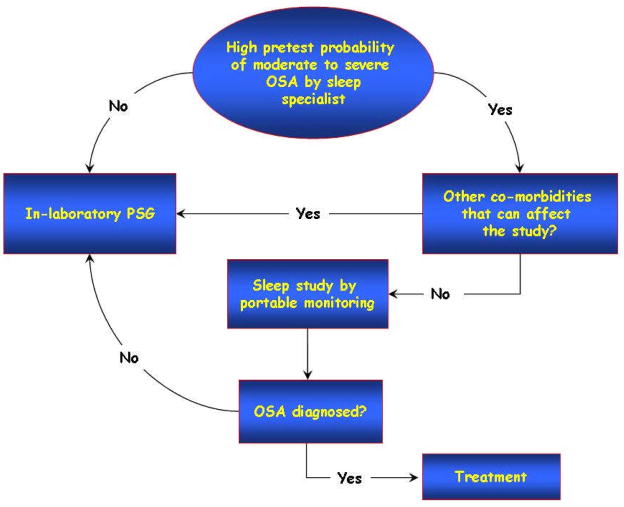
This review summarizes the recent literature on the epidemiology of adult obstructive sleep apnea (OSA) from various population-based studies. Despite methodologic differences, comparisons have yielded similar prevalence rates of the OSA syndrome in various geographic regions and amongst a number of ethnic groups. Risk factors for OSA including obesity, aging, gender, menopause, and ethnicity are analyzed. We also provide discussion on adverse medical conditions associated with OSA including hypertension, stroke, congestive heart failure, coronary artery disease, cardiovascular mortality, insulin resistance, and neurocognitive dysfunction. Finally with the progression of the global obesity epidemic, we focus on the economic health care burden of OSA and the importance of recognizing the largely undiagnosed OSA population with emphasis on strategies to improve access to diagnostic resources.
Conflict of interest statement
Figures
References
-
- Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA. 2006;295:1549–1555. - PubMed
-
- Finkelstein EA, Ruhm CJ, Kosa KM. Economic causes and consequences of obesity. Annu Rev Public Health. 2005;26:239–257. - PubMed
-
- Hensrud DD, Klein S. Extreme obesity: a new medical crisis in the United States. Mayo Clin Proc. 2006;81:S5–10. - PubMed
-
- Haslam DW, James WP. Obesity Lancet. 2005;366:1197–1209. - PubMed
-
- Kapur V, Strohl KP, Redline S, Iber C, O’Connor G, Nieto J. Underdiagnosis of sleep apnea syndrome in U.S. communities. Sleep Breath. 2002;6:49–54. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical