

Morbidity of en bloc resections in the spine
- PMID: 19690899
- PMCID: PMC2899819
- DOI: 10.1007/s00586-009-1137-z
Morbidity of en bloc resections in the spine
Abstract
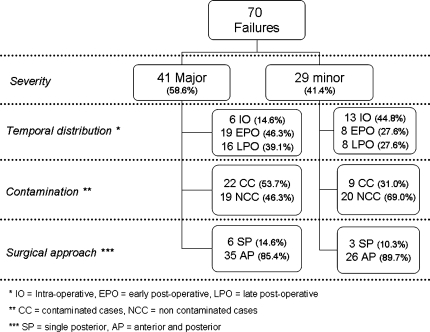
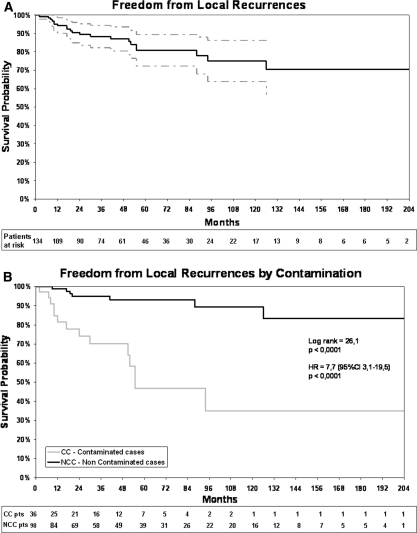
The morbidity of surgical procedures for spine tumors can be expected to be worse than for other conditions. This is particularly true of en bloc resections, the most technically demanding procedures. A retrospective review of prospective data from a large series of en bloc resections may help to identify risk factors, and therefore to reduce the rate of complications and to improve outcome. A retrospective study of 1,035 patients affected by spine tumors-treated from 1990 to 2007 by the same team-identified 134 patients (53.0% males, age 44 +/- 18 years) who had undergone en bloc resection for primary tumors (90) and bone metastases (44). All clinical, histological and radiological data were recorded from the beginning of the period in a specifically built database. The study was set up to correlate diagnosis, staging and treatment with the outcome. Oncological and functional results were recorded for all patients at periodic, diagnosis-related controls, until death or the latest follow-up examination (from 0 to 211 months, median 47 months, 25th-75th percentile 22-85 months). Forty-seven on the 134 patients (34.3%) suffered a total of 70 complications (0.86 events per 100 patient-years); 32 patients (68.1%) had one complication, while the rest had 2 or more. There were 41 major and 29 minor complications. Three patients (2.2%) died from complications. Of the 35 patients with a recurrent or contaminated tumor, 16 (45.7%) suffered at least one complication; by contrast, complications arose in 31 (31.3%) of the 99 patients who had had no previous treatment and who underwent the whole of their treatment in the same center (P = 0.125). The risk of major complications was seen to be more than twice as high in contaminated patients than in non-contaminated ones (OR = 2.52, 95%CI 1.01-6.30, P = 0.048). Factors significantly affecting the morbidity are multisegmental resections and operations including double contemporary approaches. A local recurrence was recorded in 21 cases (15.7%). The rate of deep infection was higher in patients who had previously undergone radiation therapy (RT), but the global incidence of complications was lower. Re-operations were mostly due to tumor recurrences, but also to hardware failures, wound dehiscence, hematomas and aortic dissection. En bloc resection is able to improve the prognosis of aggressive benign and low-grade malignant tumors in the spine; however, complications are not rare and possibly fatal. The rate of complication is higher in multisegmental resections and when double combined approach is performed, as it can be expected in more complex procedures. Re-operations display greater morbidity owing to dissection through scar/fibrosis from previous operations and possibly from RT. The treatment of recurrent cases and planned transgression to reduce surgical aggressiveness are associated with a higher rate of local recurrence, which can be considered the most severe complication. In terms of survival and quality of life, late results are worse in recurrent cases than in complicated cases. Careful treatment planning and, in the event of uncertainty, referral to a specialty center must be stressed.
Figures

References
-
- McDonnell MF, Glassman SD, Dimar JR, Puno HMR, Johnson JB. Perioperative complications of anterior procedures of the spine. J Bone Joint Surg Am. 1996;78:839–847. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
