

Endoscopic surgery on the thoracolumbar junction of the spine
- PMID: 19693549
- PMCID: PMC2899720
- DOI: 10.1007/s00586-009-1124-4
Endoscopic surgery on the thoracolumbar junction of the spine
Abstract
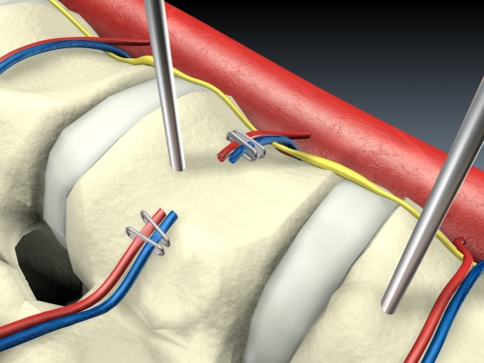
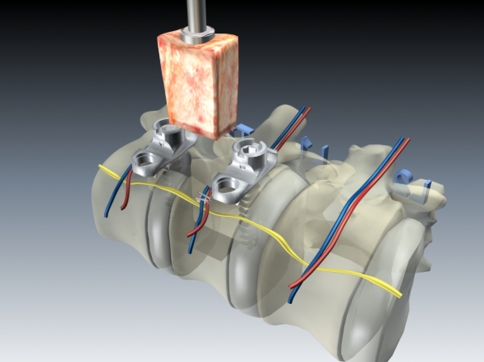
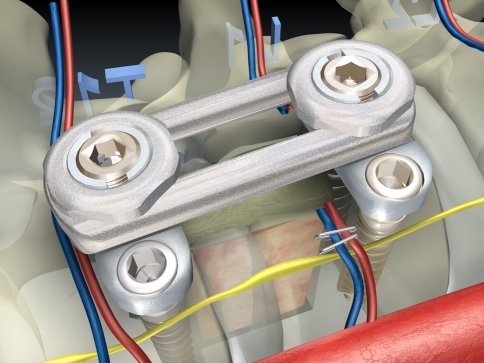
The thoracolumbar junction is the section of the truncal spine most often affected by injuries. Acute instability with structural damage to the anterior load bearing spinal column and post-traumatic deformity represent the most frequent indications for surgery. In the past few years, endoscopic techniques for these indications have partially superseded the open procedures, which are associated with high access morbidity. The particular position of this section of the spine, which lies in the border area between the thoracic and abdominal cavities, makes it necessary in most cases to partially detach the diaphragm endoscopically in order to expose the operation site, and this also provides access to the retroperitoneal section of the thoracolumbar junction. A now standardised operating technique and instruments and implants specially developed for the endoscopic procedure, from angle stable plate and screw implants to endoscopically implantable vertebral body replacements, have gradually opened up the entire spectrum of anterior spine surgery to endoscopic techniques.
Figures
















References
-
- Beisse R, Potulski M, Bühren V. Endoscopic techniques for the management of spinal trauma. Eur J Trauma. 2001;27:275–291.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
